Nomenclature of the veins of the lower limbs : An international interdisciplinary consensus statement

Nomenclature of the veins of the lower limbs : An international interdisciplinary consensus statement
SUMMARY
An agreement on anatomic terminology is the foundation for a common language in medical science and for an effective exchange of information. A thorough review of the literature has shown need for revision and extension of the official terminologia anatomica with regard to the veins of the lower limb.
The foundation of this consensus document was laid by the faculty at a precongress meeting of The Fourteenth World Congress of the International Union of Phlebology (IUP), held in Rome on September 8-9, 2001, under the auspices of the IUP, the International Federation of Associations of Anatomists (IFAA), and the Federative International Committee on Anatomical Terminology (FICAT).
The official names of some veins have been changed according to the guidelines of the FICAT. In addition, previously unnamed veins have received names relevant to their anatomy and clinical significance. Some of the terminology recommendations are innovative, but were judged to be correct by members of the committee.
BACKGROUND
Anatomy of the venous system forms the basis of clinical phlebology and is crucial to the correct evaluation and appropriate treatment of venous disorders. The current official anatomical nomenclature, Terminologia Anatomica (TA)1 has well served anatomists and clinicians involved in investigation and treatment of venous diseases. Deficiency in the nomenclature of the veins of the lower limbs, however, became obvious as knowledge accumulated about their physiology and pathophysiology. In addition, clinicians introduced and used names not present in the TA. Incorrect interpretation of these names led to confusion and even to inappropriate treatment of venous disease. For example, the main deep vein of the thigh, named the “superficial femoral vein” by some clinicians has been erroneously considered to be a superficial vein. This has led to failure to treat deep vein thrombosis.2 In current usage, the abbreviation “LSV” can represent either long saphenous vein or the lesser saphenous vein.3 This has led to confusion as to which vein was being referred to. In addition, the official anatomical nomenclature has had an inadequate listing of perforating veins, saphenous vein collaterals, tributary veins, and some of the deep veins. Several of these unlisted veins are reasonably constant in location and connections. They need an official name to obtain terminologic conformity.
OBJECTIVE
The need for a revision and an extension of the Terminologia Anatomica with respect to the veins of the lower limbs has stimulated the development of this consensus document. The aim of this project was to offer an internationally acceptable venous anatomical terminology that would satisfy both anatomists and clinicians. Another goal was to avoid any confusion for the clinical practitioner.
The foundation of this consensus document was laid by the faculty at a meeting held in Rome, on September 8-9, 2001, during The Fourteenth World Congress of the International Union of Phlebology (IUP), under the auspices of the IUP, the International Federation of Associations of Anatomists (IFAA) and the Federative International Committee on Anatomical Terminology (FICAT). Input to the document was also solicited from experts not present at the meeting: G. B. Agus (Italy), E. Brizzio (Argentina), J. Caprini (USA), A. Cavezzi (Italy), D. Creton (France), J. Dortu (France), C. Feied (USA), C. Gillot (France), M. P. Goldman (USA), W. Hach (Germany), J. Hobbs (UK), E. Mendoza (Germany), G. I. Mozes (USA), A. A. Ramelet (Switzerland), V. C. Ruckley (UK), I. Staelens (Belgium), J. Staubesand (Germany), F. Stillo (Italy), P. Thibault (Australia), J. P. Van der Stricht (Belgium).
In this consensus document, the names of some veins have been changed taking into account the past practice of the FICAT.1 Previously unnamed veins receive names relevant to their anatomy and clinical significance. Eponyms, which are not part of the official anatomical terminology, have been excluded for the most part but a few well-known names have been retained and they are indicated in brackets to assist in identification.
PRELIMINARY DEFINITIONS
The anatomy of the veins of the lower limbs is extremely variable. Nevertheless, there is order in the variability.
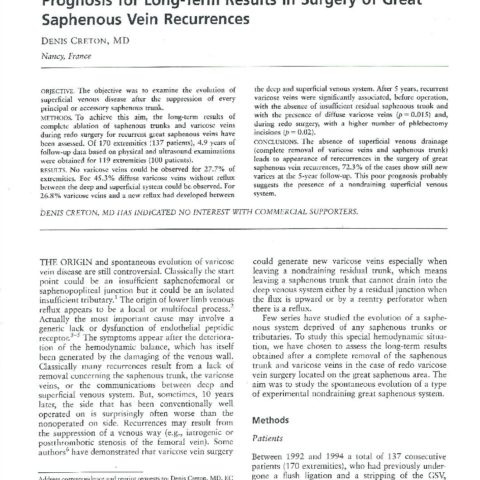
The veins of the lower extremities are divided into three systems: the superficial, the deep, and the perforating venous systems. These are located in two main compartments: the superficial compartment and the deep compartment (Fig 1).
The deep compartment is bounded by the muscular fascia and contains deep veins. The superficial compartment is bounded deeply by the muscular fascia and superficially by the dermis. In English, it would formerly have been said that the tissue between the deep fascia and dermis was superficial fascia. However, it emerged that the term fascia superficialis meant different things in English, Italian, French, and German,4 so the term was dropped and the current international term for the tissue is tela subcutanea whose English equivalent term is subcutaneous tissue. The subcutaneous tissue contains the saphenous veins and their tributaries, in addition to accessory and communicating veins.
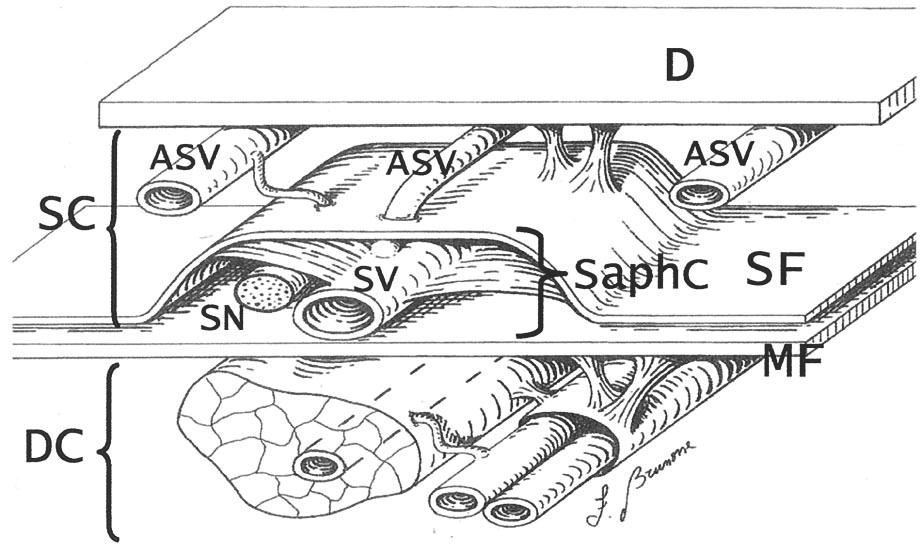
Within the superficial compartment, ultrasound technology has revealed and traditional anatomical investigations have confirmed a separate saphenous compartment. 4,5 This saphenous compartment is bounded superficially by an hyperechoic saphenous fascia and deeply by the muscular fascia of the limb. The saphenous fascia is that portion of the membranous layer of the subcutaneous tissue6 that overlies the saphenous veins (Figs 1 and 2) and their origins or roots (the marginal veins of the foot and the dorsal venous arch). In the past, the membranous layer of the subcutaneous tissue has been referred to by many inappropriate synonyms that should be abandoned: superficial fascia, Colles or Scarpa fascia, subcutaneous pseudofascia, superficial layer of the deep fascia, among others. The saphenous compartment contains the saphenous veins, accompanying arteries, and nerves. Saphenous tributaries, and accessory, collateral and communicating veins lie external to this compartment.7
The accessory saphenous veins are venous segments that ascend parallel to the saphenous veins, either anterior, posterior or more superficial with respect to the main trunk (Fig 1). This term should include all so-called collateral veins, which represent parallel pathways of alternative flow.8
The term perforating veins is reserved for those veins that perforate the muscular fascia to connect superficial veins with deep veins.9 The term communicating veins is reserved for those veins that interconnect with other veins of the same system.9
Fig. 1
The saphenous compartment (SaphC) is bound superfi- cially by the saphenous fascia (SF) and deeply by the muscular fascia (MF) and contains the saphenous veins (SV) accompanied by the saphenous nerve (SN). The accessory saphenous veins (ASV) lie external to this compartment, close to the dermis (D). SC, Superficial compartment; DC, deep compartment.
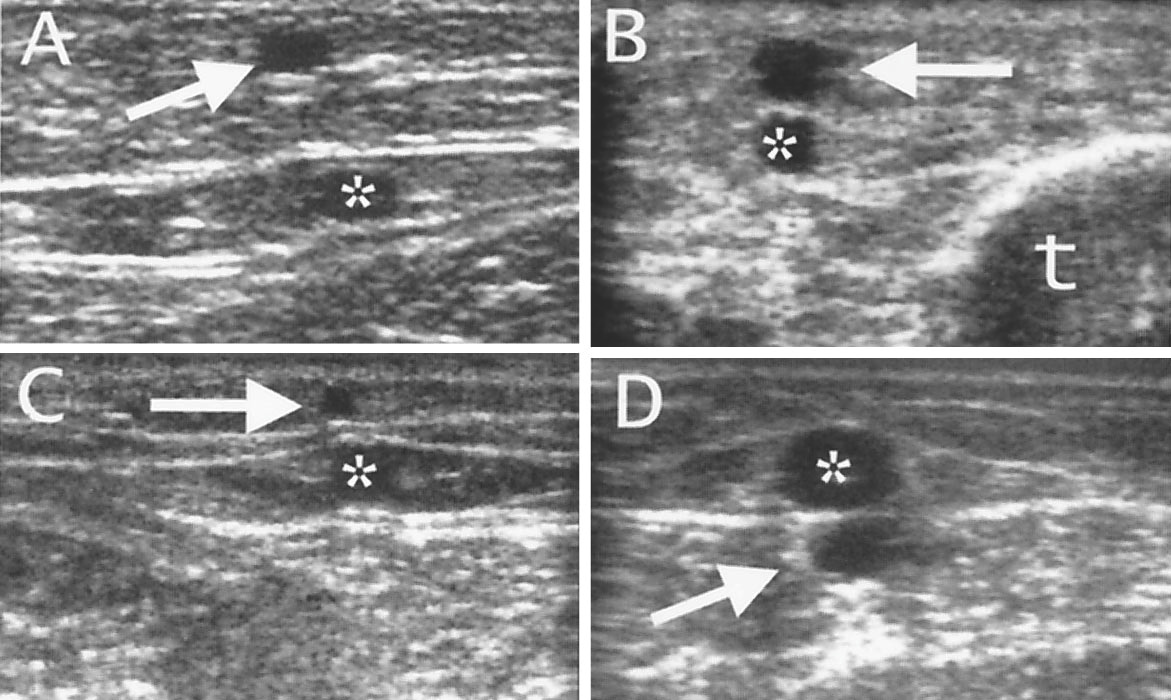
Fig. 2
Sonography of the saphenous compartment (white arrows) along the great saphenous vein at the thigh (A) and at the leg (B) and along the small saphenous vein at the calf (C) and in the distal lower leg (D). Sonography clearly demonstrates that the saphenous veins are enwrapped by two hyperechoic fasciae. Note in B, the posterior accessory saphenous vein (*) and the tibia (t).
SUPERFICIAL VEINS
The names of a few superficial veins have been changed from those in the official Terminologia Anatomica, the list of which has been extended by adding the names of a few anatomically and clinically relevant veins (Table I).
The term great saphenous vein (vena saphena magna), abbreviated as GSV should be used instead of terms such as long saphenous vein (LSV), greater saphenous vein, and internal saphenous vein. The omission of long saphenous vein is recommended so as to remove confusion caused by the abbreviation LSV, which could represent either the long saphenous vein or the lesser saphenous vein.3 Similarly, the term small saphenous vein (vena saphena parva) abbreviated as SSV, should be used instead of the terms short, external, or lesser saphenous vein.
The term confluence of superficial inguinal veins (confluens venosus subinguinalis) corresponds to the veins of the saphenofemoral junction (SFJ). This is termed Crosse by many clinicians. It also corresponds to the Venenstern unter dem Leistenband of German anatomists.10
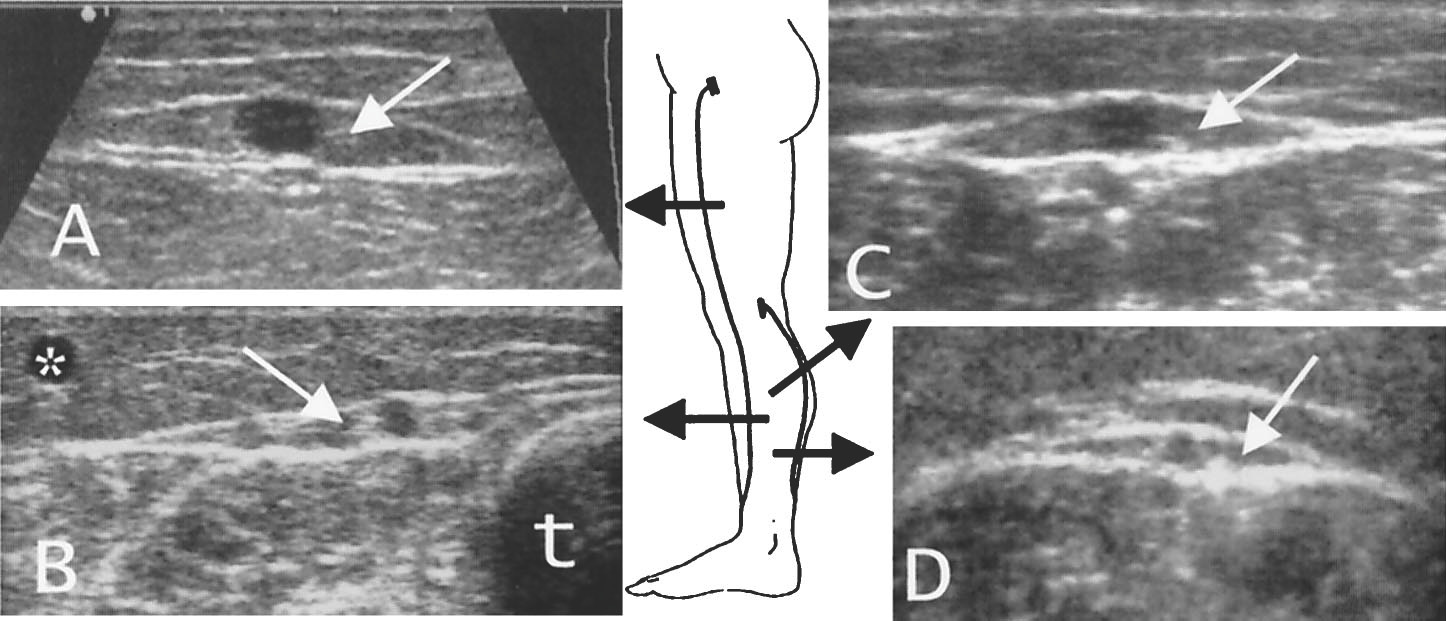
The term anterior accessory great saphenous vein (vena saphena magna accessoria anterior) indicates any venous segment ascending parallel to the GSV and located anteriorly, both in the leg and in the thigh.11(Fig 3, A).
The term posterior accessory great saphenous vein (vena saphena magna accessoria posterior) indicates any venous segment ascending parallel to the GSV and located posteriorly, both in the leg and in the thigh.12 (Fig 3, B). The leg segment corresponds to the so-called Leonardo’s vein or Posterior arch vein.
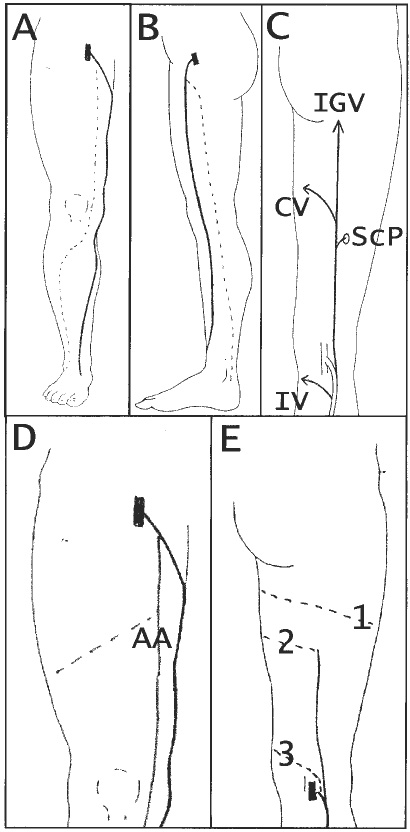
The term superficial accessory great saphenous vein (vena saphena magna accessoria superficialis) indicates any venous segment ascending parallel to the GSV and located more superficially above the saphenous fascia, both in the leg and in the thigh.13(Figs 4, A and B).
The cranial extension of the small saphenous vein (extensio cranialis venae saphenae parvae) courses in the groove between the biceps femoris and semimembranosus muscles (Fig 3, C). This vein has been called “femoropopliteal vein.”14 A cranial extension of the SSV that communicates with the GSV via the posterior thigh circumflex vein is often termed the vein of Giacomini.
The superficial accessory small saphenous vein (vena saphena parva accessoria superficialis) ascends parallel to the SSV and is located more superficially, above the saphenous fascia15 (Fig 4, C).
The anterior thigh circumflex vein (vena circumflexa femoris anterior) is a tributary vein of the GSV (or of the anterior accessory great saphenous vein) ascending obliquely in the anterior thigh.16 It may originate from the lateral venous system (Fig 3, D).
The posterior thigh circumflex vein (vena circumflexa femoris posterior) is a tributary vein of the GSV (or of the posterior accessory great saphenous vein), which ascends obliquely in the posterior thigh. This vein may originate in the SSV, in its cranial extension, or in the lateral venous system.17(Fig 3, E).
One or more intersaphenous vein(s) (vena(e) intersaphena(e)) course obliquely at the calf to connect the SSV with the GSV18 (Fig 3, C).
The lateral venous system (systema venosa lateralis membri inferioris) is extended on the lateral thigh and leg.19 It represents the remnant of the embryonic vena marginalis lateralis.
In TA, all the veins of the foot were listed as superficial veins. They should be identified according to their topographic location. It is important to note that the dorsal venous arch and the lateral and medial marginal veins course into the foot extension of the saphenous compartments. 20
Fig. 3
A, The course of the anterior accessory great saphenous vein (dotted line) is parallel and more anterior to the great saphenous vein (black line). B, The course of the posterior accessory great saphenous vein (dotted line) is parallel and more posterior with respect to the great saphenous vein (black line). C, The cranial extension of the small saphenous vein (black line) ends in the inferior gluteal vein (IGV) and can be connected to a sciatic perforator (ScP) or to the great saphenous vein via the posterior thigh circumflex vein (CV). One or more intersaphenous veins (IV) connect the small and great saphenous veins at the calf. D, The anterior thigh circumflex vein (dashed line) ascends obliquely in the anterior thigh to reach the anterior accessory great saphenous vein (AA) or the great saphenous vein. E: The posterior thigh circumflex vein (dashed lines) originates from the lateral venous plexus (1), or from the cranial extension of the small saphenous vein (2) or directly from the small saphenous vein (3). It courses obliquely in the posterior thigh toward the great saphenous vein.
Table I: Superficial veins
*1998.
| Terminologia anatomica* | Proposed terminology |
|---|---|
| Greater or long saphenousvein | Great saphenous vein |
| Superficial inguinal veins | |
| External pudendal vein | External pudendal vein |
| Superficial circumflex vein | Superficial circumflex iliac vein |
| Superficial epigastric vein | Superficial epigastric vein |
| Superficial dorsal vein of clitoris or penis | Superficial dorsal vein of clitoris or penis |
| Anterior labial veins | Anterior labial veins |
| Anterior scrotal veins | Anterior scrotal veins |
| Accessory saphenous vein | Anterior accessory great saphenous vein |
| Posterior accessory great saphenous vein | |
| Superficial accessory great saphenous vein | |
| Smaller or short saphenous vein | Small saphenous vein |
| Cranial extension of the small saphenous vein | |
| Superficial accessory small saphenous vein | |
| Anterior thigh circumflex vein | |
| Posterior thigh circumflex vein | |
| Intersaphenous veins | |
| Lateral venous system | |
| Dorsal venous net of the foot | Dorsal venous network of the foot |
| Dorsal venous arch of the foot | Dorsal venous arch of the foot |
| Dorsal metatarsal veins | Superficial metatarsal veins (dorsal and plantar) |
| Plantar venous network | Plantar venous subcutaneous network |
| Plantar venous arch | |
| Plantar metatarsal veins | Superficial digital veins (dorsal and plantar) |
| Lateral marginal vein | Lateral marginal vein |
| Medial marginal vein | Medial marginal vein |
DEEP VEINS
The names of a few deep veins have been changed from those in the TA, and the list has been extended by adding the names of a few anatomically and clinically relevant veins (Table II).
The common femoral vein (vena femoralis communis) runs from the confluence of the femoral vein and the deep femoral vein to the external iliac vein at the inguinal ligament. The femoral vein originates from the popliteal vein at the upper margin of the popliteal fossa and courses in the femoral canal. The unauthorized term “superficial femoral vein” should not be used for this vein because it is a deep vein2 and is not in the official TA.1
The profunda femoris vein (vena profunda femoris, alternative term deep femoral vein) originates from the confluence of veins draining the muscles of the posterior and lateral thigh, the deep femoral communicating veins. The term deep vein of thigh listed in TA must be abandoned because it is nonspecific and misleading.
The deep femoral communicating veins (venae comitantes arteriae perforantium; formerly the perforating veins), are the venae comitantes (accompanying veins) of the perforating arteries that originate from the deep femoral artery. The term “perforating” veins should not be applied to these veins because it is reserved for veins connecting superficial and deep veins.9
The sciatic vein (vena ischiadica) is the main trunk of the primordial deep venous system (the axial vein of embryo). It courses close to the sciatic nerve and may assume an important role as a collateral pathway for the femoral vein.21
The term « sural veins » is not sufficient to appropriately designate the complex venous system of the calf. This should be designated as soleal veins (venae solealis), the veins of the soleus muscle22 and gastrocnemius veins (venae gastrocnemii).23 The latter are divided in medial gastrocnemius vein (vena medialis gastrocnemii), lateral gastrocnemius vein (vena lateralis gastrocnemii), and intergemellar vein (Vena intergemellaris), the vein ascending between the two heads of the gastrocnemius, just below the SSV.24 (Fig 4, D).
The term genicular venous plexus (plexus venosus genicularis) should replace the term genicular veins. At the knee, deep veins do not correspond exactly to the branches of the popliteal artery (articular arteries). They are arranged in a complex plexus of interconnecting veins.25
The deep veins of the foot are the medial plantar veins, lateral plantar veins, deep plantar venous arch, deep metatarsal veins (plantar and dorsal), deep digital veins (plantar and dorsal), and the pedal vein.
Fig. 4
The superficial accessory great saphenous vein (arrows) at the thigh (A) and in the leg (B) can be recognized in its parallel and more superficial course with respect to the Great Saphenous Vein (*); t, tibia. C, The superficial accessory small saphenous vein (arrow) overlies the small saphenous vein (*) by which it is separated by the hyperechoic saphenous fascia. D, The intergemellar vein (arrow) courses deep to the small saphenous vein (*) between the heads of the gastrocnemius.
Table II: Deep veins
*1998.
| Terminologia anatomica* | Proposed terminology |
|---|---|
| Femoral vein | Common femoral vein Femoral vein |
| Profunda femoris vein or deep vein of thigh | Profunda femoris vein or deep femoral vein |
| Medial circumflex femoral vein | Medial circumflex femoral vein |
| Lateral circumflex femoral vein | Lateral circumflex femoral vein |
| Perforating veins | Deep femoral communicating veins (accompanying veins of perforating arteries) |
| Sciatic vein | |
| Popliteal vein | Popliteal vein |
| Sural veins | Sural veins |
| Soleal veins | |
| Gastrocnemius veins | |
| Medial gastrocnemius veins | |
| Lateral gastrocnemius veins | |
| Intergemellar vein | |
| Genicular veins | Genicular venous plexus |
| Anterior tibial veins | Anterior tibial veins |
| Posterior tibial veins | Posterior tibial veins |
| Fibular or peroneal veins | Fibular or peroneal veins |
| Medial plantar veins | |
| Lateral plantar veins | |
| Deep plantar venous arch | |
| Deep metatarsal veins (plantar and dorsal) | |
| Deep digital veins (plantar and dorsal) | |
| Pedal vein |
PERFORATING VEINS
The perforating veins (PV; or “perforators”) are numerous and very variable in arrangement, connection, size, and distribution.26 In clinical practice, perforating veins have been associated frequently with names of authorities, often incorrectly from a historical point of view, and some-times misleading. Instead, descriptive terms designating location are preferred. Perforators are grouped on the basis of their topography, as in Table III and in Fig 5.
The perforators of the foot (venae perforantes pedis) are divided into dorsal foot perforators, with their equivalent term intercapitular veins, medial foot perforators, lateral foot perforators, and plantar foot perforators, according to their location.27
The ankle perforators (venae perforantis tarsalis) are designated in medial ankle perforators, anterior ankle perforators, and lateral ankle perforators, according tp their topography.27
The perforators of the leg (venae perforantes cruris) are divided infour main groups. The perforators of the medial leg are designated as paratibial and posterior tibial. Paratibial perforators connect the main trunk or trbutaries of the GSV with the posterior tibial veins and course close to the medial surface of the tibia. These correspond to the so-called Sherman PV (at the lower and mid leg) and Boyd PV (at the upper leg). Posterior tibial perforators (Cockett perforators)28connect the posterior accessory great saphenous vein with the posterior tibial veins. These correspond to the so-called Cockett PV. They should not be named first, second, and third. As recommended by Frank Cockett,29 they can be indicated topographically as upper, middle, and lower.
The anterior leg perforators pierce the anterior tibial compartment and connect the anterior tributaries of the GSV to the anterior tibial veins.
The lateral leg perforators connect veins of the lateral venous plexus with the fibular veins.
The perforators of the posterior leg are divided into medial gastrocnemius perforators (in the medial calf), lateral gastrocnemius perforators (in thelateral calf), intergemellar perforators (connecting the SSV with the calf veins, also called « mid-calf perforator of May »), para- Achillean perforators (connecting the SSV with the fibular veins; also called « perforator of Bassi »).
The perforators of the knee (venae perforantes genus) are designated as medial knee perforators, suprapatellar perforators, lateral knee perforators, infrapatellar perforators, popliteal fossa perforators, according to their location.
The perforators of the thigh (venae perforantes femoris) are grouped on the basis of their topography. On the medial thigh are the perforators of the femoral canal (Dodd) and the inguinal perforators, which connect the GSV (or its tributaries) with the femoral veinat the groin.
The anterior thigh perforators pierce the quadriceps femoris. The lateral thigh perforators pierce the lateral muscles of the thigh. On the posterior thigh, Perforators are designated as posteromedial thigh perforators (those piercing the adductor muscles), sciatic perforators (lying along the midline of the posterior thigh), posterolateral thigh perforators (those piercing the biceps femoris and semitendinosus muscles, also called “perforator of Hach”), and pudendal perforators.
The perforators of the gluteal muscles (venae perforantes glutealis) are divided in superior, mid, and lower perforators.29
Fig. 5
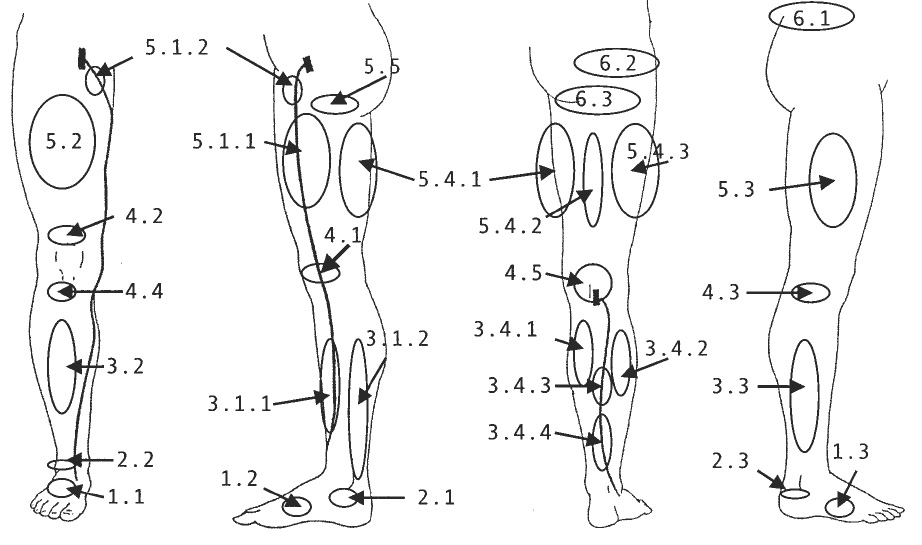
Schematic representation of the topography of the main groups of perforating veins (PVs). Foot PVs: 1.1, dorsal foot PV; 1.2, medial foot PV; 1.3, lateral foot PV. Ankle PVs: 2.1, medial ankle PV; 2.2, anterior ankle PV; 2.3, lateral ankle PV. Leg PVs: 3.1.1, paratibial PV; 3.1.2, posterior tibial PV; 3.2, anterior leg PV; 3.3, lateral leg PV; 3.4.1, medial gastrocnemius PV; 3.4.2, lateral gastrocnemius PV; 3.4.3, intergemellar PV; 3.4.4, para-achillean PV. Knee PVs: 4.1, medial knee PV; 4.2, suprapatellar PV; 4.3, lateral knee PV; 4.4, infrapatellar PV; 4.5, popliteal fossa PV. Thigh PVs: 5.1.1, PV of the femoral canal; 5.1.2, inguinal PV; 5.2, anterior thigh PV; 5.3, lateral thigh PV; 5.4.1, posteromedial thigh PV; 5.4.2, sciatic PV; 5.4.3, posterolateral thigh PV; 5.5, pudendal PV. Gluteal PVs: 6.1, superior gluteal PV; 6.2, midgluteal PV; 6.3, lower gluteal PV.
Table III: PV, Perforator vein.
| Main groups | Subgroups |
|---|---|
| Foot perforators | Dorsal foot pv or intercapitular veins |
| Medial foot PV | |
| Lateral foot PV | |
| Plantar foot PV | |
| Ankle perforators | Medial ankle PV |
| Anterior ankle PV | |
| Lateral ankle PV | |
| Leg perforators | Medial leg PV |
| Paratibial PV | |
| Posterior tibial PV | |
| Anterior leg PV | |
| Lateral leg PV | |
| Posterior leg PV | |
| Medial gastrocnemius PV | |
| Lateral gastrocnemius PV | |
| Intergemellar PV | |
| Para-achillean PV | |
| Knee perforators | Medial knee PV |
| Suprapatellar PV | |
| Lateral knee PV | |
| Infrapatellar PV | |
| Popliteal fossa PV | |
| Thigh perforators | Medial thigh PV |
| PV of the femoral canal | |
| Inguinal PV | |
| Anterior thigh PV | |
| Lateral thigh PV | |
| Posterior thigh PV | |
| Posteromedial | |
| Sciatic PV | |
| Posterolateral | |
| Pudendal PV | |
| Gluteal perforators | Superior gluteal PV |
| Midgluteal PV | |
| Lower gluteal PV |
CONCLUDING REMARKS
A common anatomical terminology is the foundation for a common language in phlebologic sciences. Further, such a common language is important for investigation of the venous system and for accurate diagnosis and correct treatment of venous disorders. Universally accepted new terminology will facilitate effective international exchange of information.
REFERENCES
From the Department of Anatomy, University of Rome.
*Complete list of participants: Claudio Allegra (Italy), Pier Luigi Antignani (Italy), John J. Bergan (USA), Alberto Caggiati (Italy), Patrick H. Carpentier (France), Frank B. Cockett (UK), Leonardo Corcos (Italy), Andre´ Cornu-The´nard (France), Bo Eklof (USA), Michael Georgiev (Italy), Peter Gloviczki (USA), Louis Grondin (Canada), Jean Jerome Guex (France), Georges Jantet, (France), Javier Leal Monedero (Spain), Hugo Partsch (Austria), Eberhard Rabe (Germany), Stefano Ricci (Italy), Angelo Scuderi (Brasil), Jean-Franc¸ois Uhl (Fance), and Colin P. Wendell- Smith (Australia).
- Federative International Committee on Anatomical Terminology. Terminologia Anatomica. Stuttgart: Thieme; 1998.
- Bundens WP, Bergan JJ, Halasz NA, Murray J, Drehobl M. The superficial femoral vein: a potentially lethal misnomer. JAMA 1995; 274:1296-8.
- Bergan JJ. Editor’s note. Venous digest 1999;6:5.
- Caggiati A. Fascial relationships of the long saphenous vein. Circulation 1999;100:2547-9.
- Caggiati A. Fascial relationships of the short saphenous vein. J Vasc Surg 2001;34:241-6.
- Wendell-Smith CP. Fascia: an illustrative problem in international terminology. Surg Radiol Anat 1997;19:273-7.
- Caggiati A. Fascial relations and structure of the tributaries of the saphenous veins. Surg Radiol Anat 2000;22:191-6.
- Churchill’s illustrated medical dictionary. New York: Churchill Livingstone; 1994.
- Staubesand J. Remarks in summary. In: May R, Partsch H, Staubesand J, editors. Perforating veins. Mu¨nchen: Urban and Schwarzemberg; 1980.
- Staubesand J, Steel F, Li Y. The official nomenclature of the superficial veins of the lower limb: a case for revision. Clin Anat 1995:8;426-8.
- Edwards E, Robuck JD Jr. Applied anatomy of the femoral vein and its tributaries. Surg Gynecol Obstet 1934;59:916-28.
- Daseler EH, Anson BJ, Reimann AF, Beaton LE. The saphenous venous tributaries and related structures in relation to the technique of high ligation. Surg Gynecol Obstet 1947;85:53-63.
- Muller R, Joubert B. La phle´bectomie ambulatoire: de l’anatomie au geste. Paris: Editions Medicales Innothera`; 1992.
- Georgiev M. The femoropopliteal vein. Derm Surg 1996;22:57-62.
- Georgiev M. The femoropopliteal vein. Derm Surg 1996;22:57-62.
- Mercier R, Fouques PH, Portal N, Vanneuville G. Anatomie chirurgicale de la veine saphene externe. J Chir 1967;93:59-70.
- Dortu JA, Dortu J. Anatomie clinique du complexe saphe´nien a la cuisse. Phlebologie 1993;46:91-100.
- Haeger K. The surgical anatomy of the sapheno-femoral and saphenopopliteal junctions. J Cardiovasc Surg 1962;3:420-7.
- Kosinsky C. Observations on the superficial venous system of the lower extremity. J Anat 1926;60:131-42.
- Albanese AR, Albanese AM, Albanese EF. Lateral subdermic varicose vein system of the legs. Vasc Surg 1969;3:81-9.
- Ricci S. Phle´bectomie des varices du pied. Phlebologie 2000;53:223-8.
- Cherry KJ, Gloviczki P, Stanson AW. Persistent sciatic vein: diagnosis and treatment of a rare condition. J Vasc Surg 1996;23: 490-7.
- Van Limborgh J, Kwakye LB. Anatomie normale des veines sole´aires chez les personnes age´es. Phle´bologie 1975;28:273-9.
- Van der Stricht J, Staelens J. Veines musculaires du mollet. Phle´bologie 1994;47:135-43.
- Lemasle P, Lefebvre-Vilardebo M, Uhl JF, Gillot C, Baud JM, Vin F. La cartographie veineuse superficielle—considerations pratiques. Phle´bologie 2000;53:77-104.
- man RS. Varicose veins. Anatomic findings and an operative procedure based upon them. Ann Surg 1944;120:772-84.
- May R, Partsch H, Staubesand J. Perforating veins. Mu¨nchen: Urban and Schwarzenberg; 1980.
- Kuster G, Lofgren EP, Hollinshead WH. Anatomy of the veins of the Dodd H, Cockett FB. The pathology and surgery of the veins of the lower limb. Second edition. Edinburgh: Churchill Livingstone; 1976.foot. Surg Gynecol Obstet 1968;127:817-26.
- Dortu J, Dortu JA. Les veines perforantes du membre inferieur. Phle´- bologie 1994;47:167-75.
| Date | 2002 |
| Awards | J. Vasc. Surg, 2002 ; 36:416-22. Alberto Caggiati, MD, John J. Bergan, MD, FACS, FRCS (Hon), Peter Gloviczki, MD, Gorges Jantet, MD, Colin P. Wendell-Smith, MD, and Hugo Partsch, MD, an International Interdisciplinary Consensus Committee on Venous Anatomical Terminology* |