Duplex ultrasound scan findings two years after great saphenous vein radiofrequency endovenous obliteration

Duplex ultrasound scan findings two years after great saphenous vein radiofrequency endovenous obliteration
SUMMARY
Objective : To assess the clinical and duplex ultrasound scan findings in the groin and thigh 2 years after great saphenous vein (GSV) radiofrequency endovenous obliteration (RFO).
Methods : Sixty-three limbs in 56 patients with symptomatic varicose veins and GSV incompetence were treated with RFO, usually with adjunctive stab-avulsion phlebectomies, and examined at a median follow-up of 25 months, by using a color-coded, duplex sonography protocol that mandated views in at least two planes of the saphenofemoral junction (SFJ) and its tributaries and at three GSV levels in the thigh.
Results : The commonest duplex finding in the groin was an open, competent, SFJ with a <5-cm patent terminal GSV segment conducting prograde tributary flow through the SFJ (82%). Despite the presence of a total of 104 patent junctional tributaries, SFJ reflux was uncommon, affecting only five limbs. GSV truncal occlusion was observed in 90% of treated GSVs. Limited segmental treatment was successful in three limbs with a midthigh reflux source well below competent terminal and subterminal valves. Six GSV trunks had partial or no occlusion, but only one refluxed. These were anatomical RFO failures (9.5%) but were clinically improved, including the refluxing limb. Neovascularity was not identified in any groin. Thigh varicosities were observed in 12 limbs, including telangiectasias and isolated small tributary branches. New varicosities, linked to refluxing thigh perforators (two), or patent SFJ tributaries (three), were present in five limbs.
Conclusion : RFO is the ideological opposite of high ligation without GSV stripping. It leaves physiologic tributary flow relatively undisturbed, does not incite groin neovascularity, eliminates the GSV as a refluxing conduit in >90% of limbs and has a 2-year, postadjunctive phlebectomy varicosity prevalence of 7.9%, with symptom score improvement in 95% of limbs with an initial score higher than zero.
INTRODUCTION
Microprocessor-controlled radiofrequency endovenous obliteration (RFO) of the great saphenous vein (GSV) has shown results comparable to those observed with saphenofemoral junction (SFJ) ligation and GSV surgical stripping through 2 years of follow-up.1 The therapeutic concept underlying the management of the SFJ and its tributaries with RFO differs from the accepted surgical principle of complete division of the tributaries entering the GSV within several centimeters of the SFJ in that normal prograde flow in these tributaries is seen as physiological and beneficial. The RFO is begun slightly distal to the SFJ, preserving flow in the more proximal tributaries to wash the SFJ as a precaution against acute thrombus extension and, in the longer term, to avoid venous hypertension in the superficial tissues of the lower abdomen and pudendum as a potential stimulus for neovascularization.2 Persistent SFJ tributary flow should pose little problem for recurrent thigh varicosities if RFO effectively eliminates the principal superficial truncal channel in the thigh. RFO is particularly adaptable to segmental obliteration. In thighs in which the source of reflux is considerably distal to the SFJ, this principle of prograde flow preservation can be extended by obliterating only the more distal refluxing segment of the thigh portion of the GSV. This changed paradigm obliges us to continue to study the patency and flow in the SFJ and its tributaries, as well as the entire treated portion of the GSV, to define the durability and clinical affects of endovenous obliteration. This study presents color-coded duplex anatomy and flow findings and the clinical status of 63 limbs at a median 25 months after GSV RFO.
PATIENTS AND METHODS
Data regarding RFO of the GSV are being accumulated in a multicenter, international registry that now comprises more than 350 patients treated at 30 sites.1 The current study cohort consisted of 56 patients with 63 treated limbs drawn from five registry centers in Austria, France, and the United States. These sites were chosen, based on the personal observations of the first author, because they had one or more highly qualified individuals who were able to provide detailed duplex ultrasound scan assessments of the SFJ, the GSV and its tributaries, and the presence or absence of groin neovascularization according to an agreed-on, standardized assessment protocol. The patients represented consecutively treated limbs at each site in which the RFO was done without concomitant SFJ ligation with an approximate 2-year follow up. Their median age was 50 years (range, 27-74 years), and 41 (73%) of the patients were women. Each limb qualified for treatment by having symptomatic varicose veins and duplex-determined GSV incompetence, with thigh GSV diameters>2mmand >12 mm, as measured with the patient supine. The RFOs were done between January 1999 and June 2000, and the follow-up examinations were conducted from January 2001 through April 2002, with a median follow-up interval of 25 months (range, 20 to 37 months).
The principles of the Closure procedure (VNUS Medical Technologies, Inc, San Jose, Calif.) have been previously described.3,4 The RFO was begun slightly below the SFJ in 60 limbs and extended to slightly above the knee in 3 limbs, to just below the knee in 56 limbs, and to the ankle in 1. Three limbs had isolated GSV trunk incompetence distal to competent terminal and subterminal SFJ valves. In accord with the preoperative ultrasound scan findings, RFO in these limbs was begun immediately proximal to a refluxing thigh tributary, well below the SFJ, confining obliteration to the incompetent refluxing GSV segment and ending just below the knee, as previously described.2 Adjunctive stab-avulsion phlebectomies were done in 50 limbs to address established varicose clusters at the time of the RFOs, usually in the calf, but including clusters in the thigh in 19 instances. Calf varicosity sclerotherapy was performed in one limb. Subsequently, follow-up avulsion phlebectomies or sclerotherapy were done in 20 limbs for either remaining or recurrent varicosities, again generally calf, but including supplemental treatments for thigh varicosities in 11 limbs.
After obtaining written informed consent, clinical examinations were performed on all patients, assessing each treated limb according to the CEAP clinical classification and looking particularly for even small clinically apparent thigh varicosities.5-7 Leg pain, limb fatigue, and transient leg swelling were each scored from 0 to 2 for none, moderate, or severe symptoms.1
Color-coded duplex ultrasound scan examinations were performed with one of four standard color duplex systems—the ATL HDI, the ATL Apoge´e (ATL Ultrasound, Philips Medical Systems, Bothell, Wash), the Acuson Sequoia (Siemens Medical Solutions, Erlangen, Germany), or the Hitachi Katana 5 (Hitachi Medical Systems Europe, Zug, Switzerland)—with high-resolution, linear probes (>7.5 mHz) according to an agreed-on assessment protocol that dictated obtaining views in at least two planes of the SFJ and the GSV and its tributaries in the groin and at three levels in the thigh. The examinations, performed with the patient standing, used calf manual compressionrelease to provoke and quantify SFJ, tributary, and truncal vein reflux. Reflux was defined as >0.5 seconds of reverse flow.8-10 The diameters of all sonographically visible thigh varicosities were measured, and a determination was made of the origin of their retrograde flow. Tributary reflux could originate from the common femoral vein (CFV) through an incompetent SFJ or from prograde flow from the terminus of another GSV terminal-segment tributary. Manual calf compression-release was also used in searching for groin neovascularization, which was defined by the presence of new conduits not identifiable as any of the normally observed branches or variants thereof.11
Ultrasound scan findings were summarized by means of simple descriptive statistics: median, and range for continuous variables and percentages with 95% confidence intervals. Χ2 or Fisher exact tests, with continuity correction, were used for comparing proportions, with a nominal α of .05 and no adjustment for multiple testing.12
VNUS Medical Technologies, Inc, provided limited funding to offset some cost associated with follow-up duplex scans and served as the data collection center. Data analyses and interpretation, writing of the report, and the decision to submit for publication were under the absolute control of the authors.
Table I: Saphenofemoral junction anatomic and flux patterns in 60 limbs
SFJ, Saphenofemoral junction; GSV, great saphenous vein; SPS, short patent segment; LPS, long patent segment.
| n | % | 95% CI | |
|---|---|---|---|
| Complete SFJ occlusion with no flow | 5 | 8.3 | 4-18 |
| Open SFJ with short (≤5-cm) patent (GSV) segment (SPS) | 53 | 88.3 | 78-94 |
| SFJ reflux | 4 | 7.6 | 3-18 |
| No SFJ reflux | 49 | 92.4 | 82-97 |
| Open SFJ with long (>5 cm) patent (GSV) segment (LPS) | 2 | 3.3 | 1-11 |
| SFJ reflux | 1 | 50.0 | – |
| No SFJ reflux | 1 | 50.0 | – |
RESULTS
SFJ anatomy and flow.
The sonographic appearances of the SFJs are presented in Table I. The most common pattern was a patent SFJ receiving prograde flow from proximal GSV tributaries through a short (≤5-cm) patent (GSV) segment (SPS) above an obliterated GSV (Fig 1). This characterized 81.7% of the 60 limbs in which GSV RFO was begun just distal to the SFJ. The lengths of GSV proximal patency in the two long patent segment (LPS) groins were 21 and 27 cm. All SPS and LPS groins had at least one patent tributary, with the GSV segment serving as a conduit to the SFJ. SFJ reflux was present in just five limbs (8.3%) and showed no direct relationship to GSV patency length, occurring in a limb with a 0.5-cm open segment and being absent in a limb a with a 21-cm patent GSV segment.
Tributary patency and neovascularity.
The distribution and fluxes of the patent proximal GSV tributaries are presented in Table II. Duplex scanning identified 104 open tributaries in the complete group of 63 treated limbs. Reflux was observed in only eight tributaries, or 7.7%, involving seven groins (11%). Six of the seven groins with reflux involved a posteromedial or anterolateral tributary that could potentially mimic pathologic pretreatment hemodynamics. Reflux was observed in 5 of 31 (16.1%) patent anterolateral tributaries, was observed as an isolated finding in four groins, and was associated with a refluxing superficial external pudendal vein in another. In the first four instances, the reflux was limited to the proximal portion of the anterolateral tributary, but it extended along the entire course of the tributary in the fifth limb. Only one of five patent posteromedial tributaries refluxed, and it was observed as an isolated finding in that groin. Reversed SFJ flow served as the sole source of tributary reflux in four groins and as a co-contributor along with prograde flow from nonrefluxing tributaries in an additional groin. The source of reflux was not discernible in the remaining two groins. Reflux was never observed in the inferior superficial epigastric or in the superficial circumflex iliac vein.
A thorough search in all groins, particularly in those with complete SFJ occlusion, uncovered no evidence of neovascularity. Every ultrasonically visible vein could be classified as a major truncal vein or some variant of an anatomic GSV tributary.
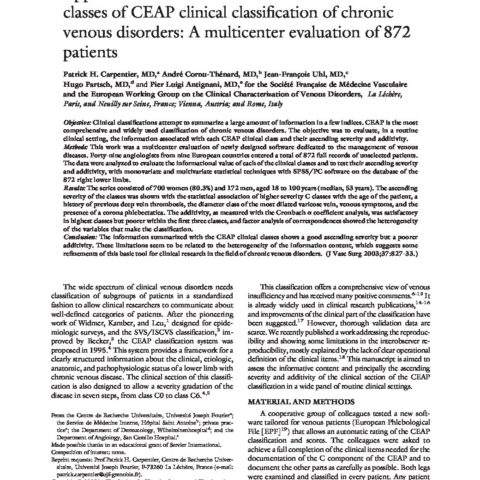
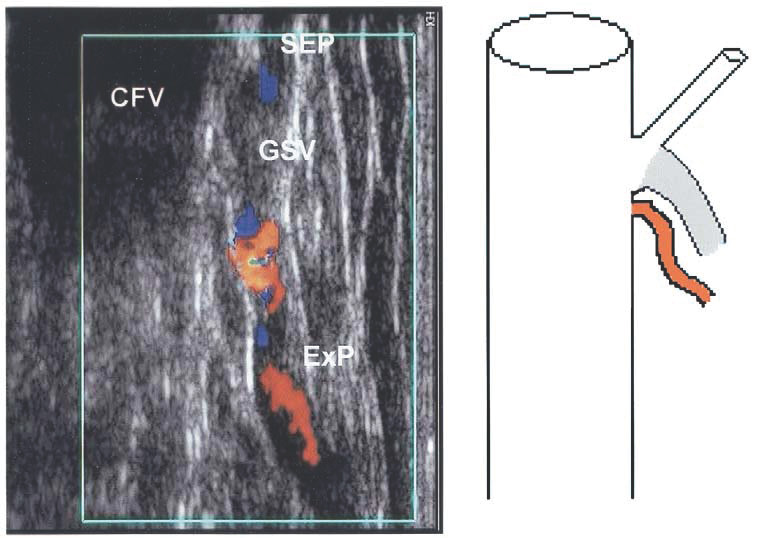
Fig. I
Sonogram and cartoon showing an open saphenofemoral junction with a short patent segment above an otherwise occluded great saphenous vein (GSV). The superficial external pudendal (SEP) vein is patent with normal, prograde flow through the SFJ. CFV, Common femoral vein.
Table II: Flow within 104 patent tributaries in 63 groins
| Tributary | Groin presence | Proportion refluxing | ||||
|---|---|---|---|---|---|---|
| n | % | 95% CI | n | % | 95% CI | |
| Inferior superficial epigastric | 33 | 52.4 | 40-65 | 0 | 0 | – |
| Superficial circumflex iliac | 15 | 23.8 | 14-36 | 0 | 0 | – |
| Superficial external pudenda | 20 | 31.7 | 21-45 | 2 | 10.0 | 3-30 |
| Anterolateral | 31 | 49.2 | 37-62 | 5 | 16.1 | 7-33 |
| Posteromedial | 5 | 7.9 | 3-18 | 1 | 20.0 | 4-62 |
| Total | 104 | 92.1* | 83-97 | 8 | 7.7 | 4-14 |
*Percentage of groins with at least one patent junctional tributary (58 of 63). CI, Confidence interval.
GSV duplex anatomy and flux in the remainder of the thigh.
As shown in Table III, anatomically successful RFO in the groin (SFJ occlusion or SPS) was accompanied by complete GSV occlusion in the thigh in 54 of 57, or 94.7%, of limbs. This was manifested sonographically either by complete disappearance of the GSV or by a hyperechogenic GSV without Doppler detectable flow (Fig 2). Selective treatment of isolated refluxing GSV segments in the mid- and distal thigh also resulted in persistent occlusion in three limbs, making the RFO anatomical success rate for GSV occlusion 57 of 63, or 90.5%, after 2 years (95% confidence interval [CI], 81-96).
Two limbs had incomplete distal-thigh GSV occlusion with narrowed irregular lumens and substantial wall thickening. Neither vein refluxed. Three GSVs had round unrestricted lumens and no wall thickening in some portion of the treated area. One of these limbs was the only limb in the study with a refluxing treated GSV trunk. The reflux came from an incompetent femoral canal (Hunterian) perforating vein, distal to a reflux-negative, SPS groin and an intervening occluded segment. One GSV had an unrestricted lumen and no wall thickening throughout its entire treated length. This GSV had only prograde flow through the SFJ and competent thigh perforators.
Of the five limbs with SFJ reflux, four had complete GSV occlusion distal to a SPS or LPS groin. The fifth limb had partial occlusion with luminal narrowing distal to a SPS groin and an intervening occluded segment. CFV reflux flowed through the SFJ into a junctional tributary, but the partially occluded GSV segment was reflux-free.
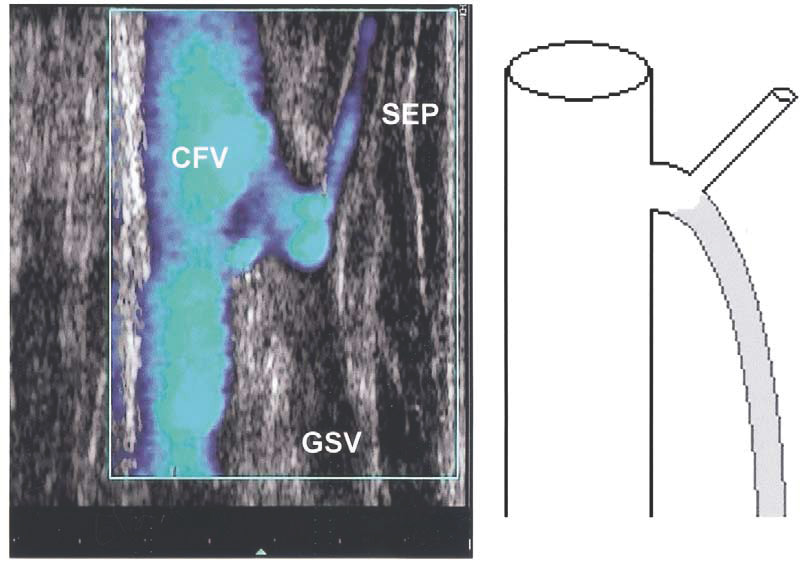
Fig. II
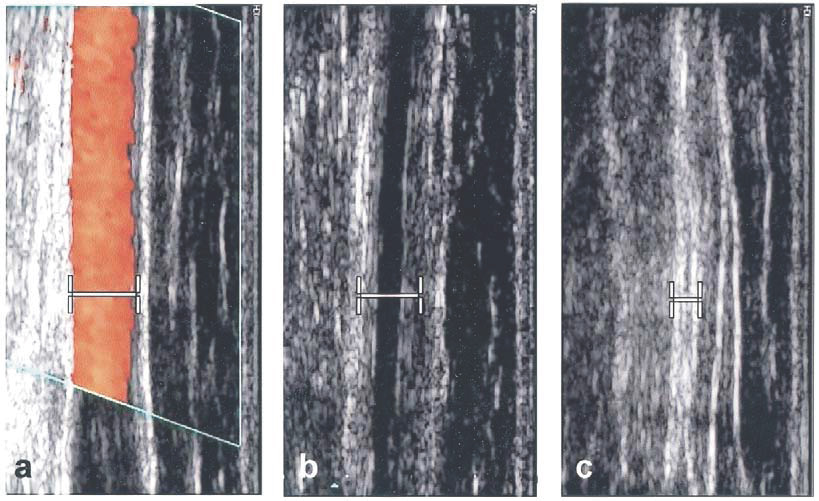
a, Pretreatment duplex image showing midthigh great saphenous vein reflux. Note diameter markers. b, Same vein level at 6 mo, showing diameter reduction, vein wall thickening, and a narrow, irregular, echolucent lumen without flow. c, Same level at 2 years, now seen as a featureless hyperechogenic stripe with further diameter shrinkage and no discernible lumen.
Table III: Duplex great saphenous vein anatomy and flow in the remainder of the thigh according to groin status
SFJ, Saphenofemoral junction.
| GSV trunk morphology | |||||
|---|---|---|---|---|---|
| Hyperecogenic | Partial or no occlusion | Total | |||
| Invisible | Without flow | No reflux | Reflux | ||
| Complete SFJ occlusion | 4 | 0 | 1 | 0 | 5 |
| Open SFJ with short patent segment | 47 | 3 | 2 | 1 | 53 |
| Open SFJ with long patent segment | 0 | 0 | 2 | 0 | 2 |
| Untreated | 3 | 0 | 0 | 0 | 3 |
| Total | 54 (85.7%) | 3 (4.7%) | 6 (9.5%) | 63 | |
Clinical status.
Varicose veins were observed in 12 limbs, or 19% of those examined. Among them, nine limbs had only telangiectases or small tributary branches. Two of the latter were related to thigh perforators, and the varicosities in the other three limbs were clearly linked to groin tributaries, making the postadjunctive phlebectomy varicosity prevalence 7.9% (95% CI, 3-17). The reflux patterns of the varicosities associated with groin tributaries were the following :
- Posterior-thigh varicosities filling from a refluxing superficial external pudendal vein connected directly to the CFV with complete SFJ occlusion (Fig 3).
- terior-thigh varicosity reflux from the CFV through the SFJ into a refluxing posteromedial tributary in a SPS, reflux-positive groin.
- Anterior-thigh varicosities filling from the CFV both through the SFJ and from pelvic escape tributaries that refluxed through the superficial external pudendal and anterolateral tributaries in a SPS, reflux-positive groin.
Table IV shows the pretreatment CEAP clinical class and symptom scores and the 2-year symptom scores according to the RFO anatomic result. Anatomically successful and unsuccessful 2-year symptom scores were similar, as symptomatic improvement characterized 94.6% (95% CI, 85-98) of the limbs with an initial score >0, including the limb with GSV truncal reflux. The CEAP-6 limb’s active ulcer healed within 45 days and remained healed at 2 years. Groin and mid- to distal thigh duplex anatomy and flow were descriptors of the treated veins’ reaction to RFO but were not reliable indicators of the presence or severity of leg symptoms.
Fig. 3
Sonogram and cartoon showing superficial external pudendal (SEP) vein prograde flow through an ultra short, patent, great saphenous vein (GSV) segment and a refluxing external pudendal (ExP) vein, originating directly from the common femoral vein (CFV), that bypasses a competent saphenofemoral junction to fill posterior thigh varicosities.
Table IV: Pretreatment CEAP and symptoms scores and symptomatic improvement as a function of anatomically successful radiofrequency endovenous obliteration and abolition of great saphenous vein (GSV) reflux
*≤5-cm patent proximal GSV or saphenofemoral junction occlusion and mid- and distal-thigh GSV disappearance, or hyperechogenicity without Doppler detectable flow. †Limb with GSV truncal reflux.
| Pretreatment | 2-year symptom scores | Unsuccessful (n = 6) |
||||
|---|---|---|---|---|---|---|
| CEAP class | Limbs | Symptom score | Limbs | All Limbs | Successful (n = 57)* |
|
| 0 | 0 | 0 | 7 | 53 | 48 | 5 |
| 1 | 2 | 1 | 12 | 6 | 5 | 1† |
| 2 | 39 | 2 | 20 | 4 | 4 | 0 |
| 3 | 4 | 3 | 18 | 0 | 0 | 0 |
| 4 | 17† | 4† | 4 | 0 | 0 | 0 |
| 5 | 0 | 5 | 2 | 0 | 0 | 0 |
| 6 | 1 | 6 | 0 | 0 | 0 | 0 |
| Median | 2 | Median | 0 | 0 | 0 | 0 |
DISCUSSION
Posttreatment groin duplex assessments revealed ultrasound scan patterns that differed from those observed and expected after GSV surgical stripping. When RFO was begun just distal to the SFJ, obliteration equivalent to standard flush ligation was observed in >10% of groins. In 81.7% of these limbs, the SFJ remained patent with a terminal short-patent segment that served as a conduit for normal physiologic flow from one or more patent tributaries through the SFJ. CFV reflux through an incompetent SFJ toward a tributary was observed in only four of these 52 groins, and in just one of two limbs, with longer, patent GSV segments as has been reported previously.1,2,13 Because all of these limbs had GSV reflux before treatment, many must have had SFJ incompetence as well. The low incidence of SFJ reflux when the junction remains patent indicates that GSV obliteration often restores terminal valve competence, presumably through reduced flow and diameter reduction. The natural history of terminal valve competence with an incompetent subterminal valve and GSV reflux is for the terminal valve competence to persist. 14 This indicates that the reflux-negative, short-patent segment groins have a good probability of persisting just as they are now. Reflux was not observed in the tributaries draining the lower abdominal wall, and they most often affected the anterolateral tributary, which, along with the posteromedial tributary, has the potential to reproduce adverse pretreatment hemodynamics if it becomes part of a reflux path.
RFO GSV commonly produces the opposite anatomical situation to high ligation without stripping, where neovascularization is very frequent and is thought to be the primary cause for recurrent reflux and varicose veins.15 Surgical wound healing and frustration of SFJ tributary physiologic drainage are potential stimuli to the formation of new connecting veins between the deep and superficial systems.16 Both are integral components of high ligation with or without GSV stripping, particularly with extended high ligation.17 Both are circumvented by RFO of the GSV and its common anatomic outcome. Neovascularity was not found in short- or long-patent segment groins, but neither was it seen in groins with complete SFJ occlusion and no tributary access to the CFV, perhaps because there were only five groins with this anatomy.
Ultrasonic disappearance of the GSV trunk, as observed in 86% of the treated GSVs, marks complete vein wall involution. Earlier stages in the maturing biologic process engendered by RFO are seen as a hyperechogenic stripe with a narrow, contorted, echolucent lumen with no flow (Fig 2). There is no tendency to recanalize once this stage is reached. Early on, partial occlusion with wall thickening and persistent flow might progress to complete occlusion, but at 2 years, it is evidence of anatomic treatment failure, as was seen in six of the study veins. It is not necessarily a bad clinical outcome, and the GSV usually becomes reflux free, as it did in five of the six veins with partial or no occlusion.
Similarly, as exemplified by the three limbs with recurrent varicosities linked to SFJ tributary reflux, an initially good anatomic result does not guarantee a good cosmetic outcome. Several factors are operative here. In one limb, anterolateral tributary reflux came from the CFV through both the SFJ and pelvic escape tributaries that refluxed through superficial external pudendal veins. This pattern indicates pelvic congestion. In two other limbs, the varicosities received flow from midthigh perforators. Nevertheless, persistent anterolateral and posterolateral tributary patency poses a potential hazard for reflux-induced recurrent varicosities, as happened in two limbs in this study. Should further observation reveal similar cases, it would be prudent to treat prominent anterolateral and, perhaps, prominent posteromedial tributaries, particularly if they already reflux, with RFO in conjunction with treatment of the GSV.
GSV reflux without SFJ incompetence has been reported to account for 33% to 47% of refluxing GSVs.18-20 It is noteworthy that the only refluxing treated GSV in this study received its flow from an incompetent femoral canal perforator. Given color-coded duplex imaging’s accuracy in determining the source of reflux and RFO’s adaptability to segmental treatment, limited obliteration may be an appropriate consideration when it can encompass all identifiable reflux sources and varicose conduits while preserving physiologic prograde flow in the healthy portions of the super- ficial system. The three study limbs with isolated GSV trunk incompetence that received specific segmental treatment have continuing subterminal and terminal valve competence, no treated segment patency, and no new secondary reflux, attesting to the potential merits of this approach.
In conclusion, sonographic patterns following RFO are different from those after high ligation and GSV surgical stripping. RFO commonly preserves physiologic tributary flux and tends to restore SFJ competence. It also appears to be less prone to inciting neovascularization and more adaptable to segmental truncal vein treatment. The principal cause of recurrent thigh reflux and varicosities after this treatment is linked to the potential for reflux in the anterolateral and posteromedial thigh tributaries. This indicates that a particularly large, or already refluxing, variant should be considered for RFO in conjunction with obliteration of the incompetent GSV. Despite the fact that groin status, tributary patency, and degree of GSV occlusion were not well correlated with clinical symptoms at 2 years, we believe that new endovenous treatments merit repetitive, detailed, duplex imaging and urge those interested in laser ablation and echo foam occlusion to adopt a similar follow-up strategy.
We thank Jean-Luc Bosson, MD, PhD, from the Clinical Investigation Center of Grenoble University Hospital, Grenoble, France, for statistical advice and analysis and Michel Nuta, MD, from VNUS Medical Technologies, for his assistance in data retrieval.
REFERENCES
- From the Division of Vascular Medicine, Grenoble University Hospital,a the Vein Institute of New Jersey,b Espace Chirurgical Ambroise Pare´,c Nancy, France, the Reno Vein Clinic,d the Hautklinik LKH, University of Graz,e and the Department of Surgery, University of Colorado Health Sciences Center.f
- Merchant RF, DePalma RG, Kabnick LS. Endovascular obliteration of saphenous reflux: a multicenter study. J Vasc Surg 2002;35:1190-6.
- Pichot O, Sessa C, Chandler JG, Nuta M, Perrin M. Role of duplex imaging in endovenous obliteration for primary venous insufficiency. J Endovasc Ther 2000;7:451-9.
- Chandler JG, Pichot O, Sessa C, Schuller-Petrovic S, Kabnick L, Bergan JJ. Treatment of primary venous insufficiency by endovenous saphenous vein obliteration. Vasc Surg 2000;34:201-14.
- Manfrini S, Gasbarro V, Danielsson G, Norgren L, Chandler JG, Lennox AF, et al. Endovenous management of saphenous vein reflux. J Vasc Surg 2000;32:330-42.
- Porter JM, Monetta GL. An international Consensus Committee on Chronic Venous Disease. Reporting standards in venous disease: an update. J Vasc Surg 1995;21:635-45.
- Kistner RL, Elkof B, Masuda EM. Diagnosis of chronic venous disease of the lower extremities: the CEAP classification. Mayo Clin Proc 1996;119:483-6.
- Ad Hoc Committee, American Venous Forum. Classification and grading of chronic venous disease in the lower limbs; a consensus statement. J Cardiovasc Surg 1997;38:437-41.
- Labropoulos N, Giannoukas A, Delis K, Mansour A, Kang S, Nicolaides A, et al. Where does venous reflux start? J Vasc Surg 1997;26:736-42.
- De Maeseneer M, Tielliu I, Van Schil P, De Hert S, Eyskens E. Phlebology 1999;14:118-22.
- Myers K, Wood S, Lee V, Koh P. Variation of connections to the saphenous systems in limbs with primary varicose veins: a study of 1,481 limbs by duplex ultrasound scanning. J Phlebol 2002;2:11-17.
- Fischer R, Linde N, Duff C, Jeanneret C, Chandler JC, Seeber P. Late recurrent saphenofemoral junction reflux after ligation and stripping of the greater saphenous vein. J Vasc Surg 2001;34:236-40.
- Newcombe, Robert G. Two-sided confidence intervals for the single proportion: comparison of seven methods. Stat Med 1998;17:857-72.
- Sybrandy J, Wittens C. Initial experiences in endovenous treatment of saphenous vein reflux. J Vasc Surg 2002;36:1207-12.
- Cappelli M, Molino Lova R, Ermini S. Incompetence of the terminal valve of the sapheno-femoral junction and incompetence of the saphenous vein trunk: is it the same disease? Int Angiol 2001;20(suppl 1):98.
- Jones L, Braithwaite BD, Selwyn D, Cooke S, Earnshaw JJ. Neovascularisation is the principal cause of varicose recurrence: results of a randomised trial of stripping the long saphenous vein. Eur J Vasc Endovasc Surg 1996;12:442-5.
- Fischer R, Chandler JG, De Maeseneer M, Frings N, Lefebvre- Vilarbedo Earnshaw JJ, et al. The unresolved problem of recurrent saphenofemoral reflux. J Am Coll Surg 2002;195:80-94.
- Chandler JG, Pichot O, Sessa C, Schuller-Petrovic S, Osse FJ, Bergan JJ. Defining the role of extended saphenofemoral junction ligation: a prospective comparative study. J Vasc Surg 2000;32:941-53.
- poulos N, Leon M, Nicolaides AN, Giannoukas AD, Volteas N, Chan P. Superficial venous insufficiency: correlation of anatomic extent of reflux with clinical symptoms and signs. J Vasc Surg 1994;6:953-8.
- Abu Own A, Scurr JH, Coleridge Smith PD. Saphenous reflux without incompetence at the sapheno-femoral junction. Br J Surg 1994;10: 1452-4.
- Pichot O, Sessa C, Bosson JL. Duplex imaging analysis of the long saphenous vein reflux: basis for strategy of endovenous obliteration treatment. Int Angiol 2002;21:333-6.
| Date | 2004 |
| Awards | J Vasc Surg 2004 ;39 :189-95 Olivier Pichot, MD,a Lowell S. Kabnick, MD,b Denis Creton, MD,c Robert F. Merchant, MD,d Sanja Schuller-Petroviæ, MD, PhD,e and James G. Chandler, MD,f Grenoble, France; Morristown, NJ; Nancy, France; Reno, Nev; Graz, Austria; and Denver, Colo |