A non draining saphenous system is a factor of poor prognosis for long-term results in surgery of great saphenous vein recurrences
A non draining saphenous system is a factor of poor prognosis for long-term results in surgery of great saphenous vein recurrences
ABSTRACT
Objectives : To study the evolution of superficial venous disease after the suppression of every principal or accessory saphenous trunk.
Methods : To achieve this aim, the long-term results of complete ablation of saphenous trunks and varicose veins during re-do surgery for recurrent great saphenous veins have been assessed. Re-do surgery for a recurrent varicofemoral junction (RVFJ) (new communication between the femoral vein and varices in the groin) (table 1) was carried out. This new communication situated on the former crossectomy stump was re-ligated, and a complete removal of varicose veins was also performed. Out of 170 extremities treated on 137 patients, a 4.9 year-follow-up data based on physical and ultrasound examinations were obtained for 119 extremities on 100 patients.
Results : Results shows that no varicose veins or incompetent superficial veins could be observed for 27.7% of extremities. For 45.3% of extremities, diffuse varicose veins without reflux between the deep and superficial system could be observed, more frequently between 2 continguous areas (groin-thigh, thigh-calf) rather than distant areas (groin-calf) (p=0.001) For 26.8% of extremities, varicose veins and a new site of incompetence had developed between the deep and superficial venous system (for 5 extremities, there was formation of another RVFJ). After five years, recurrent varicose veins were significantly associated, in pre- operative, with the absence of insufficient residual saphenous trunk and with the presence of diffuse varicose veins (p=0.015) and, during re-do surgery, with a higher number of phlebectomy incisions (p =0.02).
Conclusions : The absence of superficial venous drainage leads to appearance of re-recurrences in the surgery of great saphenous vein recurrences. After complete removal of varicose veins and no saphenous trunk left, 72.3% of the cases show still new varices at five years follow-up. This poor prognosis probably suggests the presence of a non draining superficial venous system.
INTRODUCTION
Origin and spontaneous evolution of varicose vein disease is still controversial. Classically the start-point could be an insufficient sapheno femoral or sapheno popliteal junction but it could be an isolated insufficient tributary [1]. The origin of lower limb venous reflux appears to be a local or multifocal process [2]. Actually the most important cause may involve a genetic lack or dysfunction of endothelial peptidic receptor [3-5]. The symptoms appear after the deterioration of the hemodynamic balance which has itself been generated by the damaging of the venous wall. Classically many recurrences result from a lack of removal concerning the saphenous trunk, the varicose veins or the communications between deep and superficial venous system. But, sometimes, ten years later, the side, which has been conventionally well-operated on, is surprisingly often worst than the non-operated on side. Recurrences may result from the suppression of a venous way (e.g. iatrogenic or post-thrombotic stenosis of the femoral vein). Some authors [6] have demonstrated that varicose vein surgery could generate new varicose veins especially when leaving a non draining residual trunk, which means leaving a saphenous trunk that cannot drain into the deep venous system either by a residual junction when the flux is upwards or by a re-entry perforator when there is a reflux.
Few series have studied the evolution of a saphenous system deprived of any saphenous trunks or tributaries. In order to study this special hemodynamic situation we have chosen to assess the long-term results obtained after a complete removal of the saphenous trunk and varicose veins in the case of re-do varicose vein surgery located on the great saphenous area. The aim was to study the spontaneous evolution of a type of experimental non draining great saphenous system.
METHODS
Patients
Between 1992 and 1994 a total of 137 consecutive patients (170 extremities), who had previously undergone a flush ligation and a stripping of the GSV, underwent a re-do surgery consisting, at the same time, in a re-operation for recurrent saphenofemoral incompetence, complete ablation of varicose veins and stripping the residual saphenous trunks. No documentation or post-operative records were available to say nothing of data about pre and post operative exams.
These patients were retrospectively classified from clinical records as C2, C3, or C4 in accordance with the CEAP criteria. Patients showing previous deep venous thrombosis or clinical signs of deep venous insufficiency were excluded as well as patients with insufficient short saphenous vein. Each patient underwent a Doppler ultrasonography (done by the same technician) before the procedure. Preoperative marking was performed with the use of a Doppler ultrasound study of the femoral region (Hitachi EUB 555 [7.5 Mhz] transducer; Ecoscan, Les Ulis, France; and Esaote AU 530 [10 Mhz] transducer; Biomedica, Leperreux, France).
All the patients showed a residual stump in the area of the sapheno femoral junction corresponding to an incomplete removal of the previous sapheno-femoral junction This new connection showed a reflux exceeding 1 second, calculated during the pumping of the calf muscle. A recurrent varico-femoral junction (RVFJ) (new communication between the femoral vein and varices or superficial veins) (figure 1) provided a connection between the femoral vein and an insufficient residual saphenous trunk or accessory saphenous trunk. The definition of residual trunk was, indifferently the genuine trunk in its anatomical subfascial position [7] or an accessory saphenous trunk.
The patients who had undergone a re-do procedure showed one of the following anatomical types of recurrence (figure 2) : type 1, presence of a saphenous trunk with a direct connection to the femoral vein by means of a residual stump (junction through a tributary or intact sapheno femoral junction); type 2, presence of a saphenous trunk with an indirect connection to the femoral vein by means of newly formed vessels in the groin; type 3, presence of an isolated saphenous trunk with the proximal end not connected to the incompetent residual stump; and type 4, presence of a residual stump associated with diffuse varicose veins. The first three types showed a residual saphenous or accessory trunk whereas type 4 showed only diffused varicose veins. Considering the very low rate of C3/C4, the absence of C5/C6 and the absence of clinical sign and history of deep venous thrombosis routine assessment for deep-vein insufficiency was not carried out.
Surgical technique
Surgical procedures were performed under loco regional anesthesia with a femoral nerve block, injection of 50% lidocaine solution to extend the area of anesthesia to the residual varicose veins, and, if requested by the patient, an injection of midazolam and alfentanil for sedation and pain control. It was a always unilateral procedure. Eighty-two percent of patients chose to be treated as outpatients.
The operation was carried out using a lateral approach to expose the stump, as previously described, with suture ligation of the stump and burying it with a back and-forth suture of the femoral vein adventitia. A partitioning was achieved by interposition of an ePTFE patch (W.L. Gore & Associates, Flagstaff, Arizona, USA). [8]. Incompetent residual saphenous trunks and accessory trunks were stripped with a Pin-Stripper (Tüscher, Berne, Switzerland) always on the thigh, never below knee. During the same operation, varicose veins were totally removed with Muller avulsion hooks inserted through phlebectomy incisions. The number of phlebectomy incisions was recorded for each operation. Insufficient perforators connected to the varicose network were removed by means of phlebectomies. Postoperative compression was achieved by applying double class II stockings for 3 days followed by single class II elastic compression for 1 month. No patients were proposed postoperative injection sclerotherapy, however 25 of them chose it but compliance was poor.
Follow-up study
One month later a second postoperative imaging was carried out to verify that the varicose veins as well as the residual trunk had been completely removed. All the patients who had undergone re-do surgery for recurrent varicose veins since 1997 were asked to undergo a physical examination and a Doppler ultrasound study. After these tests, they were classified into 2 categories (figure 3): type A, absence of varicose veins, (C0, C1 of the CEAP classification) and type B, presence of varicose veins (C2 of the CEAP classification); then the extremities with type B results were divided into 2 subgroups:
- First, type B1, presence of visible or palpable varicose veins, exceeding 3 mm in diameter, but no reflux from the deep to the superficial veins (i.e. no reflux when performing Valsalva maneuvres and when compressing and decompressing the calf). They were venovenous shunt type R3, according to Cappelli’s definition [6] i.e., neovessels bridging the R2-R2 or R3-R3 ligature or the R2-R3 or R2-R4 compartments. The presence of a single varicose vein, even a few centimeters long, in any area -perineal, inguinal, femoral, calf, or popliteal- was considered as evidence of ongoing varicose disease in that area.
- Second, type B2 : presence of varicose veins and of another incompetent connection between the deep and superficial network with reflux during calf compression and decompression (new RVFJ, incompetent femoral perforating vein or incompetent small saphenous vein). These varices corresponded to a new venovenous shunt i.e., neovessels bridging the R1-R2 or R1-R3 compartments [9]
Data from all these patients were recorded and compiled. Statistical analyses using ?2 tests were made to evaluate : first, the relation between recurrence of varicose veins five years after re-do surgery and their location on the lower extremity (contiguous, groin-thigh, thigh-calf, and noncontiguous areas, groin-calf) and second : the relations between five-year follow-up results, patients’ ages and the number of pregnancies in female patients and third : the relations between the anatomical type of five-year follow-up new recurrence and the number of phlebectomy incisions during re-do surgery. A P value less than 0.05 was considered to represent statistical significance.
RESULTS
Between 1997 and 1999, in the context of this follow-up study, 100 patients were examined (90 women and 10 men; mean age 53.5, ranging from 26 to 72). Female patients had undergone an average of 2.5 pregnancies before re-do varicose vein surgery. No patients were pregnant after re-do surgery. No patients had vulvar or perineal veins suggesting the presence of ovarian vein incompetence. The average period of time between re-do surgery and follow-up is 4.9 years (ranging from 3 to 7 years). A total of 119 extremities (61 right legs and 58 left legs) were examined.
Before re-do surgery, 34 of the extremities had been classified with a type 1 recurrence, 23 with a type 2, 4 with a type 3, and 58 with a type 4. The average number of phlebectomy incisions was 39.9 (ranging from 5 to 92). For 33 extremities (27.7%), the follow-up examinations showed no varicose veins or incompetent veins (type A findings) ; 86 extremities showed new varicose veins, 54 extremities of them (45.3%) with type B1 findings and 32 of them (26.8%) with type B2 findings. In this last group 5 cases showed a new RVFJ. The follow-up examinations showed no saphenous trunk.
Table 1 shows the locations of new varicose veins according to the type of follow-up findings. Statistical analysis revealed that recurrence of varicose veins after re-do surgery was less likely to appear in two noncontiguous areas (groin versus lower leg, p=0.023) than in two contiguous areas (groin versus thigh, p=0.001; thigh versus lower leg, p=0.001). The presence of varicose veins in contiguous areas (thigh and lower leg) was linked to the presence of varicose veins in the groin (p=0.002 when groin varicose veins were present and p=0.012 when they were absent).
In the follow-up examinations (type A findings), no correlations could be established between the absence of varicose veins and, either the patients’ ages (p=0.221) or the number of previous pregnancies (p=0.883). Conversely, the presence of varicose veins after re-do surgery at follow-up (types B1 and B2) was significantly associated with both type 4 preoperative recurrence (p=0.015) and a greater number of phlebectomy incisions during re-do surgery (p=0.02) (Table 2).
Patients who showed a residual insufficient saphenous trunk before re-do (type 2, 3) were significantly correlated with patients with good result showing no varicose veins at the follow up examinations (type A) (Table 2).
Out of the 81 patients with type B1 or B2 findings after re-do surgery, ten of them had undergone another re-do procedure (two perforators of the popliteal fossa, an incompetence of a short saphenous vein, an incompetent thigh perforator and six phlebectomies).
DISCUSSION
The residual saphenous trunks found when recurrences occur must be missed saphenous trunks of first surgery. Retrospectively, the differentiation between a normal subfascial trunk, an accessory extra-fascial trunk and a bifid saphenous trunk [10] is difficult to establish. The complete removal of the superficial venous system (trunk, tributaries and varicose veins) in the area of the great saphenous vein could not prevent the new development of varicose veins from happening in this area.
If we consider that the « no varicose veins » result criteria are the same in this study as in Cappelli’s [6], long-term results of a complete truncular and varicosis ablation are not better than those obtained with the CHIVA method where a saphenous draining residual trunk is left, (27% of the patients without varicose veins at follow up versus 41.2% with the CHIVA method). The spreading of the varicose network and the progression of new vessels without reflux from deep to superficial veins can be considered as either signs of severe varicose disease or more probably as the hemodynamic consequences of a definitely “non draining” saphenous system. Residual varicose veins or a non draining residual saphenous trunk could induce new-vessel formation with progression, a process that stabilizes with the appearance of a re-entry communicating vein (inguinal neovascularization). The poor prognosis of the diffused varicose veins could be explained by the fact that it corresponds to an already non drained system resulting from a previous stripping.
The correlation between a greater number of incisions during re-do surgery (which is directly related to the extent of the varicose network) and recurrence of varicose veins after such surgery, suggests (Table 2) that varicose disease is sometimes serious and progressive. The same comment can be made for recurrence after re-do surgery and type 4 recurrence.
For patients of our series: the fact that non refluxing superficial new vessels were more common between 2 contiguous areas than between 2 noncontiguous areas suggests that new-vessel formation is an ongoing progressive process. The appearance of these new vessels in the inguinal region probably corresponds to the development of new drainage routes to the deep venous system. Hydrostatic pressure in these vessels may account for contiguous proximal-to-distal development, resulting in a higher rate of varicose vein occurrence in the thigh and lower leg in patients with varicose veins in the groin. Turton [11] has demonstrated the occurrence of new reflux after stripping procedures in previously normal superficial veins in 19.6% of the cases. Dysfunction may be induced by changes in the hemodynamic organization of the superficial venous system.
To summarize, since it is not possible to restore the quality of drainage of the saphenous vein system, extensive resection of varicose veins during re-do surgery is probably another reason for the relatively good long-term results obtained. Unfortunately it is likely leaving a new non draining saphenous system when removing a residual saphenous trunk may leads to new varices. Thus it is necessary to carry out a comprehensive hemodynamical exploration of a residual trunk in order not to remove a trunk which normally drains proximally into the deep system or distally through re-entry perforators.
The carrying out of recurrent surgery is rather tricky since the necessary ablation of residual saphenous trunks, often justified by the symptomatology deriving from it and the complete removal of varicose veins, justified by an aesthetic point of view, may render the superficial venous drainage all the more difficult. Nevertheless, for recurrent surgery where the saphenous trunks have already been removed, a complete ablation of the varicose vein system may be hemodynamically questionable but seems to be inevitable in order to lessen the long-term occurrence of new varicose veins. Excessive resection can prove worse than incomplete resection. More studies will be necessary to demonstrate that accurate adaptation of the venous resection to the hemodynamic dysfunction can improve the long term follow up
ACKNOWLEDGEMENTS
This study was supported by the Swiss Society of Phlebology. Statistical analyses were carried out by F. Kohler PR, Spieao, Medical University of Nancy, Nancy, France.
REFERENCES
- Creton D. Diameter reduction of the proximal long saphenous vein after ablation of a distal incompetent tributary. Dermatol Surg 1999;25:1-5.
- Labropoulos N, Giannoukas AD, Delis K, Mansour MA, Kang SS, Nicolaïdes AN, Lumley J, Baker WH. Where does venous reflux start ? J Vasc Surg 1997;26:736-42.
- Barber DA, Wang XW, Gloviczski P, Miller VM. Characterization of endothelin receptors in human varicose veins. J Vasc Surg. 1997;26:61-9.
- Hollingsworth SJ, Tang CB, Dialynas M, Barker SGE. Varicose veins : Loss of release of vascular endothelial growth factor and reduced plasma nitric oxide. Eur J Vasc Surg 2001;22:551-6
- Agu O, Hamilton G, Baker DM, Dashwood MR. Endothelin receptors in the ethiology and pathophysiology of varicose veins. Eur J Vasc Endovasc Surg 2002;23:165-71
- Cappelli M, Lova RM, Ermini S, Turchi A, Bono G, Bahnini A, Franceschi C. Ambulatory conservative hemodynamic management of varicose veins: critical analysis of results at 3 years. Ann Vasc Surg 2000; 14: 376-84.
- Ricci S, Caggiati A. Achoanatomical patterns of the long saphenous vein in patients with primary varices and in healthy subjects. Phlebology 1999;14:54-8
- Creton D, Surgery for recurrent saphenofemoral incompetence using expanded polytetrafluoroethylene patch interposition in front of the femoral vein: long-term outcome in 119 extremities. Phlebology 2002;16:93-7
- Franceschi C. Théorie et pratique de la cure conservatrice et hémodynamique de l’insuffisance veineuse en ambulatoire. Précy-sous-Thil, Edition de l’Armançon, 1988.
- Shah DM, Chang BB, Leopold PW, Corson JD, Leather RP, Karmody AM. The anatomy of the greater saphenous venous system. J Vasc Surg 1986;3:273-8
- Turton EPL, Scott DJ, Richards SP, Weston MJ, Berridge DC, Kent PJ, Kester RC. Duplex-derived evidence of reflux after varicose vein surgery: neoreflux or neovascularisation? Eur J Vasc Endovasc Surg 1999; 17: 230-3.
Figure 1
Neovascularization (NV) corresponds to a venous network located in the groin, passing sometimes through lymphatic nodes (LGN) and connected with abdominal subcutaneous veins, deep veins, insufficient residual stump (RS) and insufficient residual saphenous trunk (RST)
Figure 1
Figure 2
Classification of the anatomical types of recurrences :
- type 1 : saphenous trunk with a direct connection to the femoral vein by means of a residual stump (junction or collateral of the intact sapheno femoral junction)
- type 2 : saphenous trunk with an indirect connection to the femoral vein by means of newly formed vessels in the groin
- type 3 : isolated saphenous trunk with the proximal end not connected to the incompetent residual stump
- type 4 : residual stump associated with diffuse varicose veins.
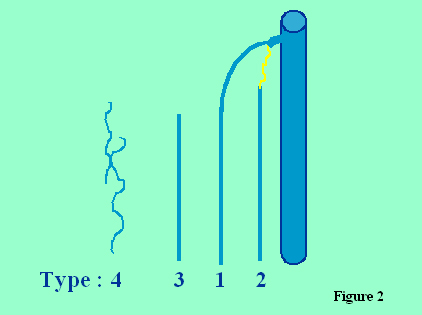
Figure 3
Classification of the results at follow-up :
- type A : absence of varicose veins, (C0, C1 of the CEAP classification)
- type B1 : presence of visible or palpable varicose veins, exceeding 3 mm in diameter, but no reflux from the deep to the superficial veins (i.e. no reflux when performing Valsalva maneuvres and when compressing and decompressing the calf) (C2 of the CEAP classification)
- type B2 : presence of varicose veins and of another incompetent connection between the deep and superficial network (C2 of the CEAP classification)
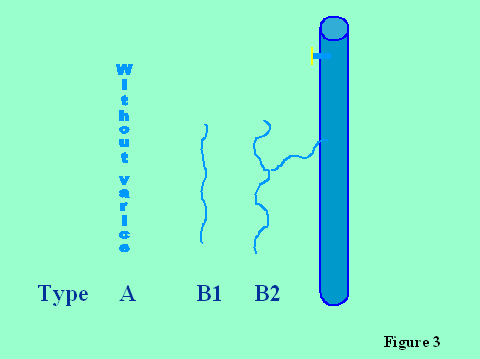
Table I
| Type (no./% of extremities) and location | No. of recurrent veins |
|---|---|
| B1 (54/62.7) | |
| Varicose veins and varicosities | 38 |
| Groin | 22 |
| Thigh | 57 |
| Lower leg | 67 |
| Thigh or lower leg | 81 |
| Popliteal fossa | 4 |
| B2 (32/35.5) | |
| Popliteal fossa | 2 SSV, 1 RSSV, 4 PPF, 1 RPPF |
| Thigh | 8 TP |
| Lower leg | 10 LP |
| Groin, thigh, lower leg | 2RVFJ, 1RVFJ+ TP, 1 RVFJ+RSSV |
| Groin | 1 RVFJ |
SSV indicates short saphenous vein; RSSV, recurrent short saphenous vein; PPF, perforator in popliteal fossa; RPPF, recurrent perforator in popliteal fossa; TP, thigh perforator; LP, leg perforators and RVFJ, recurrent varicofemoral junction (new communication between the femoral vein and varices in the groin). Type B1 indicates presence of visible or palpable varicose veins, exceeding 3 mm in diameter, but no reflux from the deep to the superficial veins and type B2, presence of varicose veins and of another incompetent connection between the deep and superficial network.
Table II
Relation between types of varicose vein recurrence assessed preoperatively and presence and absence of varicose veins at follow-up after re-do surgery, and relation between recurrence after re-do surgery and number of phlebectomy incisions made during re-do surgery
| Type of recurrence and % of all recurrences |
|||||
|---|---|---|---|---|---|
| Follow-up results | Type 1 | Type 2 | Type 3 | Type 4 | No. of incisions |
| Varicose veins present (type B1 or B2) | 29 | 12.7 | 2.3 | 55.8* | 40.12† |
| Varicose veins absent (type A) | 27.3 | 36.4 | 6.1 | 30.3 | 33† |
*p=0.015 for the difference between the percentage of varicose veins recurrences (type B1 or B2) after re-do surgery in extremities with type 4 recurrence compared with the other 3 types of recurrences.
† p=0.02 for the difference between the number of phlebectomy incisions performed during re-do surgery on patients with varicose veins at follow-up after re-do and the number of phlebectomy incisions performed on those without varicose veins at follow-up.
Type 1 indicates presence of a saphenous trunk with a direct connection to the femoral vein by means of a residual stump (junction or collateral of the intact sapheno femoral junction), type 2 : presence of a saphenous trunk with an indirect connection to the femoral vein by means of newly formed vessels in the groin, type 3 : presence of an isolated saphenous trunk with the proximal end not connected to the incompetent residual stump and type 4 : presence of a residual stump associated with diffuse varicose veins.
At follow-up, type A indicates absence of varicose veins, type B1, presence of visible or palpable varicose veins, exceeding 3 mm in diameter, but no reflux from the deep to the superficial veins and type B2, presence of varicose veins and of another incompetent connection between the deep and superficial network.
| Date | 2004 |
| Awards | Dermatol Surg 2004;30:744-9 CRETON D. |