Treatment of the incompetent great saphenous vein by endovenous radiofrequency powered segmental thermal ablation: first clinical experience
Treatment of the incompetent great saphenous vein by endovenous radiofrequency powered segmental thermal ablation: first clinical experience
Background: Radiofrequency ablation of saphenous veins has proven efficacy with an excellent side effect profile but has the disadvantage of a lengthy pullback procedure. This article reports a new endovenous catheter for radiofrequencypowered segmental thermal ablation (RSTA) of incompetent great saphenous veins (GSVs).
Methods: A prospective, nonrandomized, multicenter study was conducted to evaluate the safety, feasibility, and early clinical outcomes of RSTA of the GSV.
Results: A total of 194 patients with 252 GSVs with an average diameter of 5.7 ± 2.2 mm (range, 2.0 to 18.0 mm) received RSTA under tumescent local anesthesia. In 58 patients (29.9%), bilateral treatment (average length treated, 36.7 ± 10.8 cm) was done. The average total endovenous procedure time was 16.4 ± 8.2 minutes, and the average total energy delivery time was 2.2 ± 0.6 minutes. The corresponding endovenous fluence equivalent delivered to the proximal 7-cm vein segment was 82 ± 25 J/cm2 (range, 38 to 192). Follow-up at 3 days, 3 months, and 6 months was obtained from 250, 164, and 62 limbs, respectively. Occlusion rates were 99.6% for all three follow-up dates according to life-table analysis. The average Venous Clinical Severity Score was 3.4 ± 1.2 at 3 days, 0.9 ± 1.6 at 3 months, and 1.5 ± 1.8 at 6 months compared with 3.9 ± 2.0 at baseline.
Conclusion: Radiofrequency segmental thermal ablation is feasible, safe, and well tolerated. ( J Vasc Surg 2008;47:151-6.)
INTRODUCTION
Endovenous thermal ablation techniques, which include radiofrequency ablation (RFA) or endovenous laser treatment (ELT), are less invasive treatment options as an alternative to high ligation and stripping of the incompetent great saphenous vein (GSV), and the mid-term results of RFA and ELT suggest that endovenous thermal ablation techniques are at least as effective and durable as traditional saphenous vein surgery.1-4 Furthermore, the superiority of endovenous thermal ablation over high ligation and stripping in terms of return to normal physical activity has been indicated in randomized trials.5-7
RFA and ELT differ significantly in their mode of action of delivering thermal energy to the vein wall. Laser energy is delivered endovenously from the fiber tip and is highly focused, with temperatures of >100°C close to the fiber tip.8 RFA operates by resistive heating of the vein wall in its whole circumference, causing endovenous temperatures of 85° to 90°C. As a result of the high temperature and the focused nature of the laser beam, ELT, unlike RFA, is generally associated with vein wall perforations.8,9 This is one of the reasons why ELT is associated with more treatment-related pain and indurations during the patient recovery phase compared with RFA.10 However, the mode of action of RFA causes also a significantly prolonged ablation time if compared with ELT.
To overcome the disadvantage of slower treatment but to keep the advantage of fewer side effects in the posttreatment interval, a new radiofrequency powered catheter using the principle of segmental thermal ablation was developed. This article reports the first clinical experience in 194 patients and 252 limbs treated with this novel treatment modality.
METHODS
Patients
The patients were an average ± SD age of 50.5 ± 13.6 years (range, 18 to 80 years), and 144 (74.2%) were women. Patient comorbidities were moderate; the most frequent were hypertension in 35 (18%) and thyroid disease in 19 (9.8%). Less frequent were cardiovascular disease in 3 (1.5%), peripheral arterial disease in 2 (1.0%), arthritis in 3 (1.5%), diabetes mellitus in 7 (3.6%), and severe obesity (body mass index >30) in 1 (0.5%).
The pretreatment maximum CEAP clinical class distribution is summarized in Table I. C3 or lower class comprised 82.1% of limbs. The average preprocedure Venous Clinical Severity Score (VCSS) score was 3.9 ± 2.0 (range, 1 to 11). To detect potential influences of the vessel geometry on the efficacy of the study treatment, the anatomy of the saphenofemoral junction (SFJ) was classified as funnel shape in 47.2%, cylinder shape in 37.3%, or bulbous in 14.3% of limbs. Pretreatment vein diameters measured in the supine position at 3 cm distal to the SFJ averaged 5.7 ± 2.2 mm (range, 2.0 to 18.0 mm).
Study design
This prospective, nonrandomized, multicenter study evaluated the feasibility, safety, and early clinical outcomes of RSTA of the GSV in patients with chronic venous disease. Study treatments were performed at eight different clinical sites in Germany and France after approval by local authorities and the local ethical review boards according to the Declaration of Helsinki and its later extensions. The study sites were selected by the study sponsor because of their substantial experience in endovenous thermal ablation. The centers received free catheters and technical equipment for treatment of study patients.
Data storage and data monitoring were also provided by the study sponsor. Authors had access to any of these data as requested for analysis and interpretation of study results. Written informed consent was obtained from all patients enrolled in the study, and clinical data were collected on standardized case report forms.
Inclusion criteria
Patients of different clinical stages of chronic venous disease and reflux in the GSV demonstrated by duplex ultrasound (DUS) imaging were candidates for study treatment and were further screened for study enrollment. Significant GSV reflux was defined as reflux duration of >500 ms after the Valsalva maneuver or distal augmentation while the patient was standing or in reverse Trendelenburg position. Reflux had to be demonstrated continuously from the SFJ down to the distal point of reflux. Large vein diameters were not an exclusion criterion for study enrollment Additional inclusion criteria for enrollment into the study were age 18 to 80 years, a general physical condition allowing for frequent ambulation after the procedure, and availability to complete the follow-up visits according to the study protocol. Patients who were pregnant, breast-feeding, or who had evidence of old or fresh thrombus in the vein segment to be treated were excluded from study enrollment.
Patient follow-up
During an initial phase of the study, patients (71 limbs) were followed up at 72 hours, 3 weeks, 3 months, and 6 months. After an interim analysis on treatment outcomes and side effects, the 3-week visit was found to be uninformative and was discontinued. Each follow-up visit consisted of clinical examination, the completion of a questionnaire and DUS examination of the treated limb in the reverse Trendelenburg position.
The primary study end points were occlusion of and lack of reflux in the treated vein. Vein occlusion was defined as absence of any flow from 3 cm inferior to the SFJ along the whole length of the treated vein. The 3-cm limit was selected representing the occlusion status of the proximal GSV and furthermore allowed precise evaluation with a typical 4-cm-length linear ultrasound probe. Lack of reflux had to be proved by DUS imaging using the mentioned criteria along the whole vein segment treated.
Secondary end points included the evaluation of side effects, adverse events, clinical outcomes, and patient recovery after the treatment. Patient symptoms and signs were recorded using CEAP clinical classification and VCSS.11,12 The side effects and complications associated with the procedure were recorded and analyzed. Postprocedural pain and tenderness were evaluated using an analog scale, with the minimum of 0 representing no pain and a maximum of 10 representing worst possible pain. The analog scale was used in a nonvisual fashion after explaining it to the patient. Tenderness represented the discomfort level in responding to touch or palpation and was also measured using the analog scale between 0 and 10.
Statistical analysis
Baseline characteristics such as demographics, medical history, and venous symptoms were summarized using descriptive statistics. End point analysis as performed at each follow-up. Measurable parameters were expressed as mean ± SD, and proportions were expressed as percentages and 95% confidence intervals. Data were analyzed on per-patient or per-limb, as appropriate. Patients with bilateral treatment were treated as one for data analyzed by subject. For data analyzed on a by limb, the two limbs were treated separately. Descriptive statistics was performed using Excel software (Microsoft Inc, Redmond, Wash).
Study device and procedure
A segmental heating catheter of 7F diameter (ClosureFAST catheter, VNUS Medical Technologies Inc, San Jose, Calif) consisting of a 7-cm heating element covered with lubricious material, an integrated handle, and cable that connected to the VNUS RFGPlus generator was used. The thermal element consisted of a coil that was heated by a 460 kHz AC current to a temperature of 120°C during treatment cycles with a 20-second duration. A thermocouple on the heating element provided a feedback loop to the generator to adjust the generator output power to achieve and maintain the 120°C temperature.
The procedure was totally performed under ultrasound guidance. Vein access was achieved through puncture or venae sectio at the distal point of reflux, but to confine study treatment to the portion that ran within its fascial sheath. A 0.025-inch guidewire and a dilator were used to place an introducer sheath of 7F diameter and 11 cm in length intravenously. Before introduction into the vein, the lumen of the catheter was flushed with heparinized saline and capped. The catheter tip was then advanced through the introducer sheath just inferior to the ostium of the superficial epigastric vein, or at least 1 to 2 cm below the SFJ if the superficial epigastric vein was not visible. In situations where the patient presented with tortuous or unusual vein anatomies, external leg manipulation or an optional 0.025-in guidewire (150-cm wire for the 60-cm catheter or a 260-cm wire for the 100-cm catheter) could be used to facilitate catheter advancement and placement.
The leg was elevated to an angle of about 20° to 30°, and perivenous tumescent fluid was injected manually or by use of a pump along the vein, not only to control treatmentrelated pain but also to reduce the diameter of the vein and in the same instance protect surrounding tissue from heat damage. After confirmation that the vein was adequately compressed circumferentially and that the depth of the vein was at least 1 cm below the skin surface, the final catheter tip position was verified and radiofrequency segmental thermal ablation (RSTA) treatment was started under continuous ultrasound monitoring. With external compression provided by the ultrasound probe and an additional fingertip, 20-second heating cycles were delivered. In the initial catheter position near the SFJ, a second treatment cycle was applied to increase energy dosing in this critical area. The catheter was then repositioned to the adjacent segment guided by shaft markers in 6.5-cm steps to allow a 5-mm overlap of heated vein segments. After the first segment, each successive segment was treated for only one cycle, except in the case of aneurysmal segments or near large tributaries where a second cycle might be administered at the user’s discretion.
Toward the end of the treatment, the marker on the sheath indicates when the heating coil begins to enter the sheath and the treatment should be terminated (Fig 1). After the last treatment cycle, the catheter and sheath were removed from the vein and the access site was closed, if necessary.
After treatment, the entire length of the treated vein was assessed using DUS to determine vein occlusion, eventual reflux, and vein wall thickening. Post-treatment diameters of the treated vein were recorded at 3 cm and 15 cm below the SFJ, representing the proximal and middle thigh location, respectively. Procedure variables, treatment time, and any unique anatomy, side effects, or treatment events were also recorded. Linear endovenous energy density (LEED) and endovenous fluence equivalent (EFE) were calculated as already described elsewhere.2,13 These measures, originally described for ELT, were used in an analogous fashion to describe the endovenous energy delivery of the study device.
Excentric compression was applied for 24 to 72 hours by means of plaster-fixed gauze over the course of the treated vein. Graduated stockings with a maximum compression of 30 mm Hg were recommended for 1 week. During the initial phase after treatment, this doublecompression treatment should allow ideal selective compression of the treated vein. After the intervention, patients were immediately mobilized and advised to ambulate regularly. Nonsteroidal anti-inflammatory drugs were provided to the patients as needed.
RESULTS
From April to November 2006, 194 patients (252 limbs) were treated at eight sites in Germany and France; of these, 58 (29.9%) had bilateral treatments. In 48 patients, both limbs were treated in the same session, and 10 received the treatment of their other limb during a second treatment session.
Concomitant procedures
Thirty of 252 limbs had undergone previous venous interventions, including vein stripping in 3, ligation in 1, ELT and phlebectomy in 1, RFA in 1, RFA and sclerotherapy in 1, phlebectomy, sclerotherapy in 15, and 1 was unspecified. Despite any pretreatment modality, however, all limbs showed a typical nonoccluded incompetent GSV at the time of study treatment. Additional treatments performed at the time of the study procedure were phlebectomy in 71.4% limbs and foam sclerotherapy of tributaries in 13.9%. In one limb, the incompetent anterior accessory saphenous vein was treated with the segmental thermal ablation catheter concomitantly with the GSV ablation. During the study follow-up period, one additional limb had phlebectomy and 18 limbs received sclerotherapy for persisting varicose tributaries; however, how much—or if at all—these adjuvant measures contributed to the good reported occlusion rates remains unclear.
Delivery of thermal energy
The total average endovenous procedure time measured from catheter insertion to catheter removal, including the time for the administration of tumescent anesthesia, was 16.4 ± 8.2 minutes. Total average energy delivery time during segmental thermal ablation was 2.2±0.6 minutes (range, 1 to 4 minutes). Patients were treated with an average of 6.7 ± 1.7 thermal ablation cycles, and the average vein length treated was 36.7 ± 10.8 cm.
Data on energy dose delivered were available in 63 limbs treated during the early phase of the study. The average linear endovenous energy density delivered was 116.2 ± 11.6 J/cm (range, 71.4 to 143.3 J/cm) along the proximal 7-cm vein segment next to the SFJ and 68.2 ± 17.5 J/cm (range, 17.3 to 132.7 J/cm) along the remainder of the vein. Even more interesting, the endovenous fluence equivalent (EFE) calculated from the same data set at 3 cm distal to the SFJ was as high as 82 ± 25 J/cm2 (range, 38 to 192 J/cm2).
Ultrasound findings
Immediate vein occlusion after segmental thermal ablation with lack of spontaneous and augmented flow demonstrated by ultrasound was achieved in 100% of the treated veins. Vein wall thickening was evident immediately after treatment in 100% of the treated limbs.
The number of limbs due for follow-up and the number of limbs that had follow-up are presented in Table II. The vein-occlusion and reflux-free rates according to the Kaplan-Meier method were all 99.6% at 3 days, 3 months, and 6 months. The patent stump length was 1.5 plusmn; 0.7 cm at the SFJ at 6 months. A subset of 71 limbs had 3-week follow-up data that contributed no relevant additional information.
One vein exhibited flow after augmentation and reflux along the entire treated segment despite a narrowed lumen at the DUS examination on day 3. A large anterior accessory GSV was connected to the treated vein and exhibited reflux. This vein was occluded at the 3-month follow-up. One other GSV that was occluded at the 3-day follow-up showed segmental flow without reflux at the middle to lower thigh at 3 weeks and was occluded at the 3-month follow-up.
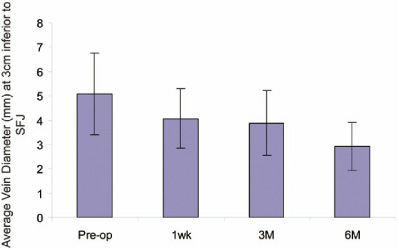
Vein diameters 3 cm inferior to the SFJ were documented at each DUS examination, and a progressive vein diameter reduction was evident, as demonstrated in Fig 2. For the limbs with follow-up data at 6 months, treated veins decreased in diameter size by 19.9% at 3 days, 26.6% at 3 months, and 43.5% at 6 months compared with the preprocedural vein diameter (P > .001, paired t test).
Clinical response and side effects
Significant patient symptom relief was observed as early as 3 days after the procedure. Limb pain, which was reported in 57.5% of limbs before treatment, decreased to 10.8% at the 3-day follow-up visit (P < .001, χ2 test). The percentage of limbs with edema decreased from 52.8% preoperatively to 3.2% at 3 days (P < .001, χ2 test). The average VCSS score was 3.4 ± 1.2 at 3 days, 0.9 ± 1.6 at 3 months, and 1.5 ± 1.8 at 6 months compared with 3.9 ± 2.0 preoperatively. It may, however, be true that a part of the improvement of edema and VCSS was due to the consequent wearing of compression stockings. Although stockings were used on 72 of 252 limbs (28.2%) before the intervention, stockings were worn after GSV ablation on 244 limbs (97%) at 3 days, 23 (14%) at 3 months, and 6 (9.7%) at 6 months.
Return to normal daily activities took place on the same day in more than half of patients, with an average ± SD of 1.0 ± 1.9 days (median, 0 days; range, 0 to 17 days).
Serious complications such as deep venous thrombosis or thermal skin injury were not observed in any study subject. Paresthesia occurred as localized patches in eight treated limbs (3.2%) during the follow-up period at the medial middle thigh region above the course of the GSV. Two limbs (0.8%) showed thrombophlebitis characterized by pain sensation and a visible reddening along the course of the treated GSV. Sole erythema was noticed in four more cases. Ecchymosis along the course of the treated GSV was present in 16 limbs after study treatment. Hematoma, defined as a three-dimensional ultrasound-detectable interstitial clot, was noticed in four limbs at the puncture site 3 days after the procedure. Skin pigmentation in the course of phlebitis or ecchymosis developed in five limbs (Table III).
Patients evaluated postprocedural pain on a scale of 0 (no pain) to 10 (worst possible pain) and 70.1% of limbs experienced no pain at any time after the procedure. The average pain score was 0.7±1.6 during the first 3 days. For patients who experienced limb pain at anytime during the follow-up period, the maximum pain score was 2.8 ± 1.6. Tenderness in response to the treatment was evaluated in similar fashion, and 67.7% of limbs experienced no tenderness at any time after the procedure. For the limbs that experienced tenderness, the maximum score was 1.9±1.2. Patient satisfaction was high: 192 of 194 patients (99.0%) would recommend the procedure to friends or relatives.
DISCUSSION
Ample clinical data have been accumulated in last several years on endovenous thermal ablation procedures, namely RFA and ELT. More recently, the concept of energy dosing during endovenous thermal ablation was recognized. With RFA, it was clear from the beginning that the catheter pullback velocity had to be slow enough to allow resistive heating of the vein wall to a target temperature of 85° to 90°C. However, because the radiofrequency power delivered by the generator was subject to regulation by a feedback loop to keep a constant temperature of 85°C at the catheter tip, measurements of the delivered energy dose to the vein were not possible under routine clinical conditions. With ELT, finally, parameters have been introduced describing the amount of delivered energy along the vein (LEED) or with respect to the inner vein wall surface (EFE).13 These parameters were determined in an analog fashion for ELT during the initial phase of this study and also with the new segmental thermal ablation catheter. The EFE at the first treatment segment was as high as 82 ± 25 J/cm2, comparable or even exceeding the EFE values reported with ELT.
The LEED is also a parameter frequently used to compare energy dosing in endovenous procedures. Timperman et al14,15 reported that 80 J/cm is required to achieve satisfactory treatment efficacy. With the ClosureFast procedure, an average of 116.2 ± 11.6 J/cm was delivered for the first 7 cm of vein near the SFJ to ensure good vein occlusion at this critical location. For the remainder of the vein, the energy dose delivered was 68.2 ± 17.5 J/cm.
As a consequence of this sufficient energy dose, a 100% ablation of reflux was achieved immediately after the procedure. With one single open vein at 3 days, life-table analysis resulted in an occlusion rate of 99.6% at 3 days, 3 months, and 6 months after the intervention. If a brief comparison of clinical outcomes at this early stage is possible at all, it may be worth stressing this significantly higher short-term occlusion rate after segmental thermal ablation compared with RFA, which was usually described at about 95%.5,16 The number of limbs at risk, however, was still small at the 6-month follow-up (Table II). Of most interest was that despite this high dosing of thermal energy, the favorable side effect profile of RFA was also demonstrated after segmental thermal ablation.
An initially pronounced and later sustained progressive shrinkage of the occluded veins may be another surrogate marker of long-term durability of segmental thermal ablation. During study follow-up, this was observed by ultrasound examination, with 19.9% vein diameter reduction as early as 3 days and 43.5% by 6 months. A few of the veins were already not identifiable by 6 months.
Another factor that may also have contributed to the excellent treatment efficacy of segmental thermal ablation was the simplicity and reproducibility of catheter pullback. Unlike the previous RFA and ELT techniques, segmental ablation is associated with a catheter that remains stationary during energy delivery. This technique avoids pullback speed variability, which can result in variable and insufficient energy dosing and thus result in inadequate treatment. Furthermore, the temperature is kept stable at 120°C during a 20-second treatment cycle, thus avoiding peak temperatures of several hundred degrees as seen with ELT ablation. This controlled heating avoids vein perforations with unintended heat damage of perivenous tissue; thus, even with high dosing of thermal energy, the procedure was well tolerated by the patients.
Patients reported no pain in >70% of their limbs at anytime after the procedure. After ELT, one can generally expect é>70% of limbs experience some degree of pain, and >50% require analgesics for pain management.2 Kabnick17 reported an average pain score of 2.2 to 2.6 on a scale of 0 to 5 after ELT.
Ecchymosis, which was observed in 6.4% limbs, was likely due to tumescent anesthesia. The incidence of phlebitis was 0.1% and paresthesia, 2.8%. This compares very favorably with the reported patient recovery profile after ELT. Ecchymosis can occur in >70% of limbs treated with ELT, likely due to vein perforation by laser energy and sometimes tumescent anesthesia.2,5 Thrombophlebitis rates of 5% to 33.3% have been reported after ELT.3,12 The occurrence of paresthesia was reported at 5% to 12% with ELT2 and previous RFA.1
With the previous RFA catheter, the slow pullback speed and the occasional need for removing the catheter to clean off the coagulum on the electrodes during the procedure were two disadvantages compared with ELT. The ClosureFast catheter completely eliminates the pullback. The average energy delivery time was 2.2 ± 0.6 minutes. To factor in other procedure steps such as tumescent infiltration and catheter repositioning, the procedure time from catheter insertion to catheter removal was 16.4 ± 8.2 minutes. This includes the learning curve and tedious ultrasound observation and documentation during the initial cases. The elimination of pullback, the short energy cycle, and the automated generator settings allowed an even, rapid treatment and dramatically simplified the procedure.
This study has some limitations. It only includes early clinical experiences from a limited number of users and only has short-term data available. Also, a control group is lacking within this study, which was focused at first on feasibility and safety. Some interesting conclusions, however, should be possible from long-term follow-up, which is currently in progress. With a wider adoption of this procedure, a variety of procedural techniques and settings could potentially affect the consistent results seen in this controlled, clinical trial setting.
CONCLUSION
Radiofrequency powered segmental thermal ablation proved to be a fast and safe procedure with close to 100% early occlusion rate of treated GSVs. Despite delivering high doses of thermal energy the method was well tolerated by the patients, who showed an insignificant side effect profile.
AUTHOR CONTRIBUTIONS
- Conception and design: TP
- Analysis and interpretation: TP
- Data collection: TP, BV JA, OG, CW, CL, OP, CS, CGS, TN, DC
- Writing the article: TP
- Critical revision of the article: TP, BV JA, OG, CW, CL, OP, CS, CGS, TN, DC
- Final approval of the article: TP, BV JA, OG, CW, CL, OP, CS, CGS, TN, DC
- Statistical analysis: TP, BV JA, OG, CW, CL, OP, CS, CGS, TN, DC
- Obtained funding: TP, BV JA, OG, CW, CL, OP, CS, CGS, TN, DC
- Overall responsibility: TP
APPENDIX
The members of the Closure Fast Study Group are Thomas Michael Proebstle, MD, MSc, and Bernadette Vago, MD, Department of Dermatology, University of Heidelberg, Germany; Jens Alm, MD, Dermatologikum, Hamburg, Germany; Oliver Göckeritz, MD, and Christian Wenzel, MD, Venenzentrum am Elsterpark, Leipzig, Germany; Christian Lebard, MD, Hospital St. Michel, Paris, France; Olivier Pichot, MD, and Carmine Sessa, MD, CHU Service de Chirurgie Vasculaire, Grenoble, France; Claus-Georg Schmedt, MD, Ludwig-Maximilian Universitaet, München, Germany; Thomas Noppeney, MD, Gemeinschaftspraxis Nürnberg, Germany; Daniel Creton, MD, Clin Ambroise Paré, Nancy, France.
REFERENCES
- Merchant RF, Pichot O; the Closure Study Group. Long-term outcomes of endovenous radiofrequency obliteration of saphenous reflux as a treatment for superficial venous insufficiency. J Vasc Surg 2005;42: 502-9.
- Proebstle TM, Moehler T, Herdemann S. Reduced recanalization rates of the great saphenous vein after endovenous laser treatment with increased energy dosing: definition of a threshold for the endovenous fluence equivalent. J Vasc Surg 2006;44:834-9.
- Min RJ, Khilnani N, Zimmet SE. Endovenous laser treatment of saphenous vein reflux: long-term results. J Vasc Interv Radiol 2003;14: 991-6.
- Sharif MA, Soong CV, Lau LL, Corvan R, Lee B, Hannon RJ. Endovenous laser treatment for long saphenous vein incompetence. Br J Surg 2006;93:831-5.
- Lurie F, Creton D, Eklof B, Kabnick LS, Kistner RL, Pichot O, et al. Prospective randomised trial of endovenous radiofrequency obliteration (closure) versus ligation and stripping (EVOLVeS): two year follow-up. Eur J Vasc Endovasc Surg 2005;29:67-73.
- Rautio T, Ohinmaa A, Perälä J, Ohtonen P, Heikkinen T, Wiik H, et al. Endovenous obliteration versus conventional stripping operation in the treatment of primary varicose veins: a randomized controlled trial with comparison of costs. J Vasc Surg 2002;35:958-65.
- Hinchliffe RJ, Ubhi J, Beech A, Ellison J, Braithwaite BD. A prospective randomised controlled trial of VNUS Closure versus surgery for the treatment of recurrent long saphenous varicose veins. Eur J Vasc Endovasc Surg 2006;31:212-8.
- Weiss RA. Comparison of endovenous radiofrequency versus 810 nm diode laser occlusion of large veins in an animal model. Dermatol Surg 2002;28:56-61.
- Proebstle TM, Lehr HA, Kargl A, Espinola-Klein C, Rother W, Bethge S, et al. Endovenous treatment of the greater saphenous vein with a 940-nm diode laser: thrombotic occlusion after endoluminal thermal damage by laser-generated steam bubbles. J Vasc Surg 2002;35:729- 36.
- Proebstle TM, Gul D, Lehr HA, Kargl A, Knop J. Infrequent early recanalization of greater saphenous vein after endovenous laser treatment. J Vasc Surg 2003;38:511-6.
- Rutherford RB, Padberg FT Jr, Comerota AJ, Kistner RL, Meissner MH, Moneta GL. Venous severity scoring: An adjunct to venous outcome assessment. J Vasc Surg 2000;31:1307-12.
- Kistner RL, Eklof B, Masuda EM. Diagnosis of chronic venous disease of the lower extremities: The “CEAP” classification. Mayo Clinic Proc 1996;71:338-45.
- Proebstle TM, Krummenauer F, Gul D, Knop J. Nonocclusion and early reopening of the great saphenous vein after endovenous laser treatment is fluence dependent. Dermatol Surg 2004;30:174-8.
- Timperman PE. Prospective evaluation of higher energy great saphenous vein endovenous laser treatment. J Vasc Interv Radiol 2005;16: 791-4.
- Timperman PE, Sichlau M, Ryu RK. Greater energy delivery improves treatment success of endovenous laser treatment of incompetent saphenous veins. J Vasc Interv Radiol 2004;15:1061-3.
- Merchant RF, DePalma RG, Kabnick LS. Endovascular obliteration of saphenous reflux: a multicenter study. J Vasc Surg 2002;35:1190-6.
- Kabnick LS. Outcome of different endovenous laser wavelengths for great saphenous vein ablation. J Vasc Surg 2006;43:88-93.
Table I: Preprocedure maximum CEAP clinical class distribution
| CEAP category | No. (%) |
|---|---|
| Data missing | 2 (0.8) |
| CEAP 1 | 2 (0.8) |
| CEAP 2 | 132 (52.4) |
| CEAP 3 | 73 (29.0) |
| CEAP 4 | 41 (16.3) |
| CEAP 5 | 1 (0.4) |
| CEAP 6 | 1 (0.4) |
Table II: Treatment efficacy
| Variable | Treatment | 3 days | 3 months | 6 months |
|---|---|---|---|---|
| Limbs due for follow-up, No. | 252 | 252 | 198 | 74 |
| Limbs with data available (limbs at risk), No. (%) | 252 (100) | 250 (99.2) | 164 (82.8) | 62 (83.8) |
| Patients due for follow-up, No. | 194 | 194 | 163 | 62 |
| Patients with data available, No. (%) | 194 (100) | 194 (100) | 132 (81.0) | 53 (85.5) |
| Vein occlusion rate per limb, %* | 100 | 99.6 | 99.60 | 99.60 |
| Reopened veins, No. | 0 | 1 | 0 | 0 |
* Kaplan-Meier method.
Table III: Complications after the procedure
| CEAP category | No. (%) |
|---|---|
| Data missing | 2 (0.8) |
| CEAP 1 | 2 (0.8) |
| CEAP 2 | 132 (52.4) |
| CEAP 3 | 73 (29.0) |
| CEAP 4 | 41 (16.3) |
| CEAP 5 | 1 (0.4) |
| CEAP 6 | 1 (0.4) |
Fig. I
Sheath marker indicates last treatment segment.

Fig. II
Average vein diameter reduction after the treatment. The error bars show the standard deviation. SFJ, Saphenofemoral junction.
| Date | 2008 |
| Awards | J Vasc Surg. 2008 ;47:151-156. Thomas Michael Proebstle, MD, MSc, Bernadette Vago, MD, Jens Alm, MD, Oliver Göckeritz, MD, Christian Lebard, MD, and Olivier Pichot, MD, for the Closure Fast Clinical Study Group, Heidelberg, Hamburg, and Leipzig, Germany; and Paris, and Grenoble, France |